Keywords
Epilepsy; Prolonged Todd paralysis
Introduction
Epilepsy is a common neurological disease characterized by recurrent seizures. These seizures can be a result of reversible dysfunction of brain including motor, sensorial, autonomic and/or impaired consciousness. These phenomena can sometimes occur in the postictal period which can be defined as the abnormal state occurring between the end of a seizure and return to baseline state. This period can be considered as the recovery process of damage caused by the seizure. The symptoms during the postictal period can vary from motor symptoms to altered cognition, psychiatric symptoms, automatic behavior, and aphasia [1]. Postictal motor symptoms are common and can range from weakness to full paralysis, which is called as Todd’s paralysis (TP). According to the literature knowledge, about 6% of patients who had tonicclonic seizures experienced TP [2]. The duration of TP may last from half an hour to 36 hours, and it is not found to be related with neither the etiology nor the seizure itself [3]. On the other hand, more prolonged postictal paralysis can occur, especially in patients with structural lesions such as tumor or stroke [4]. However, there is limited number of reports about prolonged TP. We here presented a case of TP lasted a month following secondary generalized seizures.
Case Report
A 49-year old man presented to our emergency department with sudden onset paralysis in his left limbs following recurrent generalized tonic clonic seizures (GTCS) which occurred during common cold and upper respiratory infections. His initial neurological examination revealed dysarthria and a 2/5 muscle strength in his left upper and lower limbs. He was conscious. His vital parameters were normal.
There was no systemic illness, stroke, toxin exposure, substance, alcohol and/or drug abuse in his medical history. However, he had been suffering from GTCSs and CPSs (Complex Partial Seizures) since 10 years old which began after a central nervous system infection. His seizures had a frequency of 3-4 times a month with a tendency to occur in terms of fever, and resulted with paralysis and numbness with speech difficulties which lasted approximately 2-3 days in the first years of post-infectious period. Following an antiepileptic drug (AED) regimen of phenytoin and carbamazepine (CBZ), his seizure frequency decreased to 3-4 times a year. He declared a hemiparesis following all his seizures as postictal phenomena with full recovery. However, a mild paralysis in his left limbs and dysarthria remained as sequel after the seizure occurred 5 years ago. During his follow-up visits, he suffered from skin eruptions due to CBZ, and it was switched to lamotrigine (LM). Phenytoin was ceased with slow titration and he was seizurefree since 1 year.
His recent complaint was recurrent GTCSs with left-sided paralysis; he had no non-motor symptoms like neuropsychiatric or cognitive problems. Thus he was hospitalized to our neurology clinic. There were no acute ischemic or hemorrhagic cerebrovascular lesions in his diffusion-weighted cranial magnetic resonance imaging (MRI). Thus, this hemiparesis was considered as TP. Electroencephalogram (EEG) of the patient revealed diffuse slow wave activity in theta frequency of 5-6 Hz (Figure 1). He had 3 more GTCSs following his hospitalization. Therefore, zonisamide was added to his treatment. In the 2th day of zonisamid, he was seizure-free but as angioedema occurred, zonisamide was switched to lacosamide. He was still seizurefree and there was a full recovery in angioedema. His routine blood tests including complete blood count, full biochemical screening with liver and kidney functions, electrolytes, fasting glucose levels, and thyroid function tests were normal. One week after his hospitalization, he was still suffering from left– sided hemi paralysis with 3/5 muscle strength which showed a slight recovery, and gadolinium-enhanced MRI of brain demonstrated an increased signal intensity in right temporal lobe, which was more prominent in the insular cortex, and asymmetrical changes of intensity in the right parietal-occipital lobes in axial T2-weighed cranial MRI images. These changes were found to be consistent with postictal changes (Figure 2).
Figure 1: Electroencephalogram (EEG): Diffuse slow wave activity in theta frequency of 5-6 Hz.
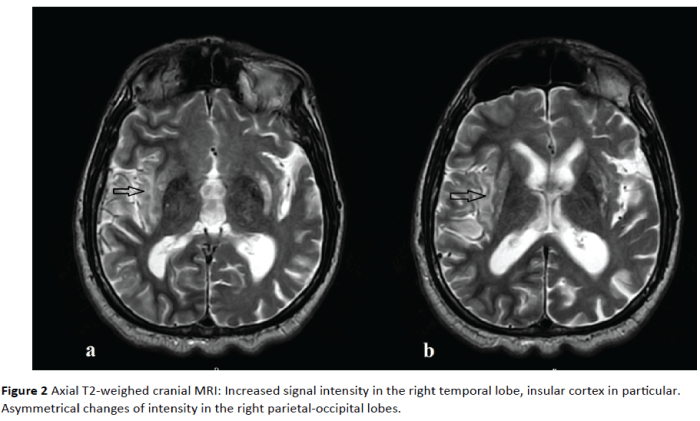
Figure 2: Axial T2-weighed cranial MRI: Increased signal intensity in the right temporal lobe, insular cortex in particular. Asymmetrical changes of intensity in the right parietal-occipital lobes.
In addition, there were signal intensity changes at mid-brain and pons which were seen iso-intense in axial T1-weighed images and hyper intense in T2-weighed cranial MRI images without any contrast. These were consistent with chronic changes and could also be seen in previous MRIs of the patient. Cranial MR angiography of the patient revealed a decreased calibration in the post-bifurcation segments of left middle cerebral artery (Figure 3).
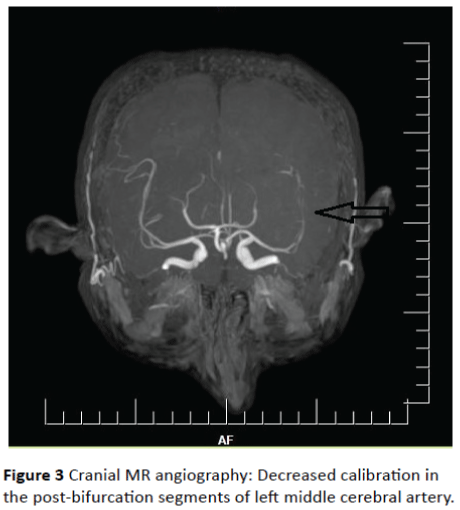
Figure 3: Cranial MR angiography: Decreased calibration in the post-bifurcation segments of left middle cerebral artery.
Since the patient was seizure-free with, LM and lacosamide, and his muscle strength showed a mild-to moderate recovery, the patient was discharged with his AED regimen, and 3/5 muscle strength in his left upper limb and 4/5 muscle strength in his left lower limb after 2 weeks. He was able to walk with support and a physical therapy program was planned for the patient. In his 1st month follow-up visit, he was still seizurefree and he was able to walk without any support.
Discussion
TP following an epileptic seizure is postictal sign and was first recognized by Bravais in 1827, who called it “hemiplegia epileptique”. It was later described by Robert Bentley Todd (1809–1860) in his clinical lectures (1854), giving his name to this phenomenon [5]. TP is a rare condition. Supporting the rarity of TP, a previous study performed in an epilepsy center among 4500 PWE reported TP in 0.64% of patients [6]. It has a slightly increased frequency in focal or lesional epileptic syndromes [1,7]. It is important to be aware that TP is not only a motor phenomenon, but also a non-motor entity including postictal altered cognition, psychiatric symptoms, automatic behavior, and aphasia. The etiology of TP is still unclear. However, the nature, duration, and severity of TP were not exactly found to be related to the duration or severity of the seizures, and the presence or absence of underlying lesions or EEG changes, as well [1].
According to our literature review, the possible mechanisms reported for the pathophysiology of TP include neuronal exhaustion from hypoxia or energy and/or substrate depletion due to a possible damage or seizure activity in a localized brain region or an underlying vascular disease leading to insufficient metabolic processes [8]. Moreover, inhibitory neuronal discharges as a result of endogenous inhibitory (possibly opioid) substances release may also be responsible for the existence of TP [8,9].
The duration of TP is generally considered to be short which can persist from half an hour to 36 hours, with a mean duration of 15 hours, and never persisted far beyond [3], whereas a longer duration was reported in stroke patients with a structural lesion in the seizure-generating hemisphere [1]. In contrast with the literature knowledge, we here reported a patient with prolonged TP which lasted a month, without any underlying acute structural or vascular lesion in brain. Similar to our case, a previous report revealed a PWE whose hemiparesis lasted 35 days [10]. As we know from the literature, brain MRI can demonstrate signal intensity alterations in the affected brain areas during the postictal period. Since it is difficult to differentiate TP from stroke, especially when there is no known history of epilepsy in the presence prolonged paralysis, we detailed the medical history of our patient and have seen that his left hemiparesis and dysarthria were not due to stroke, but remained from the TP of the seizure which occurred 5 years ago. Additionally, chronic intensity changes of brain MRI in pons and midbrain were explaining these sequels. This situation led us consider that the persistent localized neuronal exhaustion resulting from hypoxia and/or substrate depletion due to seizure activity should be considered as the underlying mechanism of recurrent and prolonged TP which may lead to stroke.
Despite the literature knowledge reporting the duration of TP as half an hour to 36 hours [3], we shared this case of TP which persisted 1 month after the cessation of seizures without any underlying acute cerebrovascular or structural lesions. This prolongation in paralysis may be related to the duration of the metabolic, biochemical and/or physiological recovery processes. On this aspect, it is important to keep in mind that prolonged paralysis following an epileptic seizure which exceeds 36 hours can still be TP, and the prolonged duration of paralysis should not be the only criteria to exclude the diagnosis of TP.
Acknowledgement
There is no funding, grand or support for the study.
Disclosure
None of the authors has any conflicts of interest to disclose.
9460
References
- Widdess WP, Devinsky O (2010) Historical perspectives and definitions of the postictal state. Epilepsy & Behavior 19: 96–99.
- Fisher RS, Schachter SC (2000) The postictal state: A neglected entity in the management of epilepsy. Epilepsy & Behavior 1: 52–59.
- Rolak LA, Rutecki P, Ashizawa T, Harati Y (1992) Clinical features of Todd's post-epileptic paralysis. Journal of Neurology, Neurosurgery, and Psychiatry 55:63-64.
- Bromfield EB, Cavazos JE, Sirven JI (2006) An introduction to epilepsy. American Epilepsy Society. West Hartford (CT).
- Werhahn KJ (2010) Weakness and focal sensory deficits in the postictal state. Epilepsy & Behavior 19: 138–139
- Kellinghaus C, Kotagal P (2004) Lateralizing value of Todd's palsy in patients with epilepsy. Neurology 62: 289–291.
- Gallmetzer P, Leutmezer F, Serles W, Assem HE, Spatt J, et al. (2004) Postictal paresis in focal epilepsies: incidence, duration, and causes. A video-EEG monitoring study. Neurology 62: 2160–2164.
- Meyer JS, Portnoy HD (1959) Post-epileptic paralysis. A clinical and experimental study. Brain 82: 162-185.
- Helmchen C, Steinhoff BJ, Dichgans M (1994) Variants of Todd's paralysis: postictal apraxia and prolonged postictal hemineglect. Nervenarzt 65: 700-703.
- Koppi S, Steger P, Peschina W, Adami P, Conca A (2008) Repetitive transcranial magnetic stimulation in a patient with atypical Todd's postepileptic paralysis. Psychiatry ClinNeurosci 62: 368.

