Steven D Hajdu* and Salah D Qanadli
Department of Diagnostic and Interventional Radiology, Lausanne University Hospital, Rue du Bugnon 46, 1011 Lausanne, Switzerland
Corresponding Author:
Steven D Hajdu
Department of Diagnostic and Interventional Radiology Lausanne University Hospital, Rue du Bugnon 46, 1011 Lausanne, Switzerland
Tel: +41-21-314 4444
Fax: +41-21-314 4443
E-mail: steven.hajdu@chuv.ch
Received date: 11 June 2016; Accepted date: 14 June 2016; Published date: 17 June 2016
Citation: Hajdu SD, Qanadli SD. Pseudoaneurysm of the Right Coronary Artery Masquerading as a Right Atrial Mass. Ann Clin Lab Res. 2016, 4:2.
A 63-year-old man under concomitant antibiotic therapy for persistent bronchitis was referred from his general practitioner for progressive dyspnea and associated chest pain. Inflammatory parameters were elevated. Serial cardiac marker enzyme levels, including Troponin I, were within normal values. Thoracic CT-angiogram and echocardiogram showed a 3 cm hyperdense mass in the right atrioventricular groove with focal subepicardial expansion along the lateral atrial wall
Case
A 63-year-old man under concomitant antibiotic therapy for persistent bronchitis was referred from his general practitioner for progressive dyspnea and associated chest pain. Inflammatory parameters were elevated. Serial cardiac marker enzyme levels, including Troponin I, were within normal values. Thoracic CT-angiogram and echocardiogram showed a 3 cm hyperdense mass in the right atrioventricular groove with focal subepicardial expansion along the lateral atrial wall (Figure 1A). Coronary CT-angiogram revealed a multilobulated, irregular luminal dilatation up to 1.5 cm in diameter of the second and third segments of the right coronary artery (RCA) surrounded by heterogeneous material suggestive of mural thrombus (Figure 1B). In the late phase, a rim of thin peripheral enhancement was visible around the adjacent pericardial hematoma (Figure 1C). The radiological findings were consistent with an unstable pseudoaneurysm (Figure 1D). The second and third portions of the RCA were surgically excised. The surgical procedure was arduous due to a perforation of the inflamed right myocardium and the patient died from right ventricular collapse due to uncontrollable hemorrhaging. A postmortem showed a neutrophilic infiltration of the resected portions of the RCA. Only a few cases of pseudoaneurysms of infectious origin have been reported and thus their associated mortality rate remains high due to delayed identification. Management of pseudoaneurysms requires individualized treatment based on a plethora of clinical data including radiological findings. Coronary CT-angiography provides superior assessment of the overall coronary anatomy allowing prompt diagnosis and appropriate surgical planning.
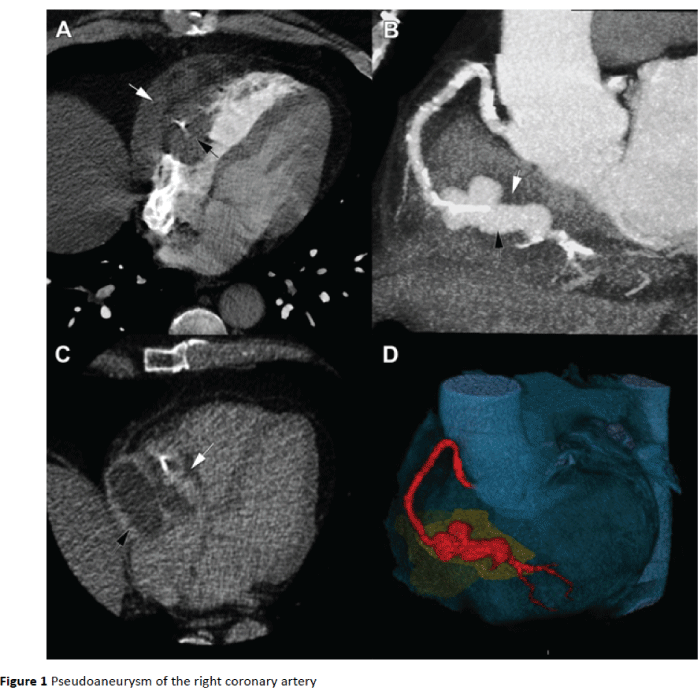
Figure 1: Pseudoaneurysm of the right coronary artery.
9641


