Keywords
Smoking, pulmonary function tests, spirometer, nonsmokers, body mass index.
Introduction
WHO estimated that 51% of adult male Jordanians are smokers, which place Jordan as number 4 in smoking among Arab countries. Smoking prevalence in females is estimated as 11% which makes Jordan as number 3 in the Arab world regarding female smokers. The country number of Jordan reached 32 in the work as cigarettes’ consumption. It is estimated to be 1832 cigarettes per person per year. The total spending per person per year on cigarettes is estimated to be 139 Jordan Dinar (JD) which ranks Jordan as the country number 62 in the world. In my opinion, these statistics are slightly underestimated and the real figures are probably higher [1].
Pulmonary function testing is a routine procedure for the assessment and monitoring of respiratory diseases [2]. Spiromeric values vary according to age, height, sex, and body size p [3,4]. Most of the studies regarding the effect of obesity on pulmonary function tests have been conducted in males, in the age group of 5 to 16 years or they have been carried out in the elderly age groups [5,6].
Tobacco has remained as one of the most important predisposing factors responsible for so many respiratory and cardiovascular diseases. Chronic Obstructive Pulmonary Diseases (COPD) has been recognized as one of the most important causes of morbidity and mortality in chronic tobacco smokers worldwide.7 COPD includes three conditions namely chronic bronchitis, emphysema and bronchial asthma which gradually cause chronic obstruction to the airflow in small airways less than 2mm in diameter. These obstructions in airways invariably affect the parameters of pulmonary function e.g. forced vital capacity (FVC), Forced Expiratory Volume in the First Second (FEV1) and Peak Expiratory Flow Rate [7]. Water pipe tobacco smoking (nargilah) is highly prevalent in Jordan, although its use is associated with male gender and upper middle income levels; also it is widespread across other sociodemographic classes. Continued surveillance and educational interventions emphasizing the harm and addictiveness of water pipe tobacco smoking may be valuable in Jordan [8].
Material and Method
A cross-sectional study was conducted at Al-Zarqa Private University-Jordan. Two hundred and thirteen of healthy smokers and nonsmoker voluntarily agreed to participate in the study. They were selected through probability sampling among the student's staff and workers who were screened through a questionnaire and spirometric testing. A structured tool of four sections was used: First: personal data includes questions related to (age, gender, faculty type, occupation) and questions related to smoking, (onset of smoking, duration, and number of cigarette per day). Second: (Anthropometric measurements) includes weight and height to body mass index (BMI). According to guidelines stated by the National Institutes of Health, weight status was classified into four categories: Underweight (BMI 18.5), normal weight (BMI between 18.5–24.9), overweight (BMI) between (25-29.9), and obese (BMI ≥30).9 Third: (Spirometric measurements) include, FVC: Forced vital capacity FEV1: Forced expiratory volume in first second, and PEFR: Peak expiratory flow rate.
Procedure
A permission to conduct the study was obtained from the university administrator. The procedure was explained and demonstrated to the subjects. Each subject was fulfilled the questioner and weighed in kilogram (kg) in indoor clothing without shoes. Standing height was measured without shoes. The subjects breathed in as deeply as possible and then blew out as hard and fast as possible to assess and monitor respiration and estimate the PEFR. Each individual made three attempts and the largest values for each parameter were used as recommended by the ATS [10].
Data of the subjects that did not match the acceptability and reproducibility criteria of ATS was discarded. The acceptability criteria of ATS includes satisfactory start of the test (extrapolated volume of less than 5% of FVC or 0.15 L, whichever is greater), minimum FVC exhalation time of 6 seconds or reasonable duration of plateau on time-volume curve, free of artifacts like coughing, glottis closure during exhalation, leak, obstructed mouth piece or early termination and end of test criteria [10].
The reproducibility criteria of ATS is that the difference among two largest FVC and FEV1 values should not exceed 0.2 L [10]. The computerized spirometer provided values with the graph for FVC, FEV1 and PEFR. All displaceable volumes were reported in liters.
Results
Data from 213 smokers and 98 nonsmokers was analyzed. Table (1): the finding included 213 subjects with mean age 25.34±7.73 years. Most of them were male (75.12%). About half of sample (53.05 %) was students. In regards to type of work, it was found that about half of sample (53.99%) was smokers with mean duration of smoking 5.82 year and mean cigarette per day 24.18. Concerning the mean of height, weight, and BMI were 176.94, 73.28, and 24.22 respectively. Also mean of spirometric values of FVC (L) FEV1 (L) FEV1/FV% PEFR were4.38, 2.23, 75.60, and 560.35 respectively.
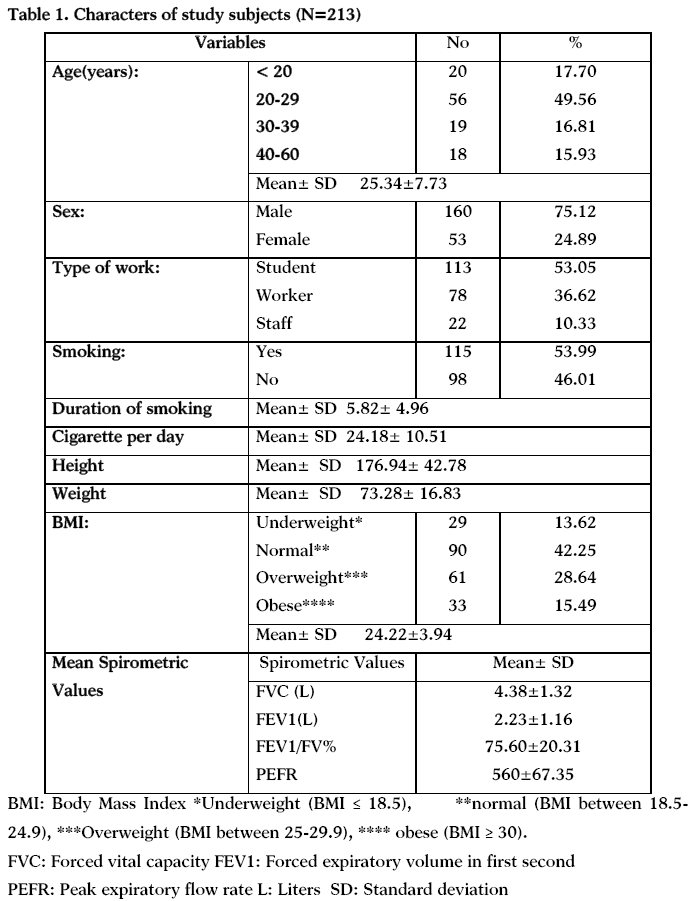
Table (2): shows that there is statistical difference between mean spirometric values FVC (L), FEV1 (L), FEV1/FEV%, PEFR) among smokers and nonsmokers.
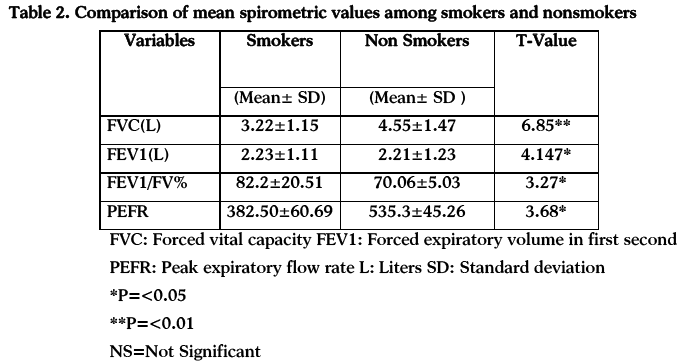
Table (3): shows that there is statistical difference between mean spirometric values FVC (L), FEV1 (L), FEV1/FEV%, PEFR) for male and female.
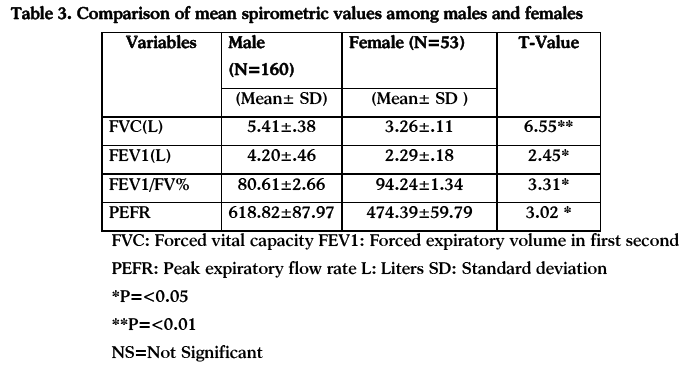
Table (4): Shows there is no statistical difference between mean spirometric values FVC (L) FEV1/FEV%, PEFR) for BMI, but FEV1 (L) there is statistical difference.
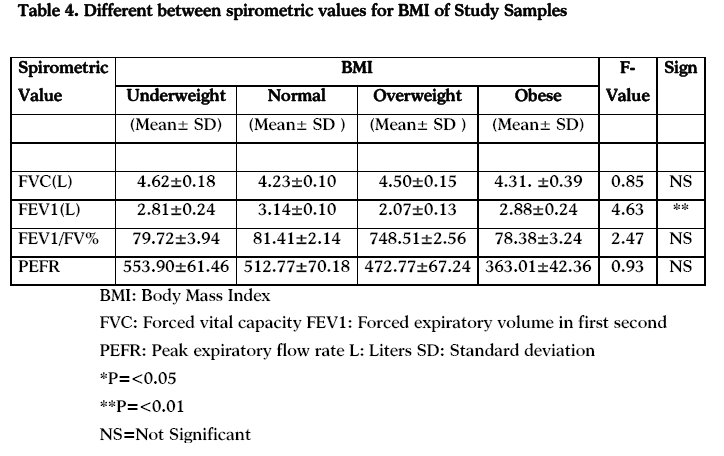
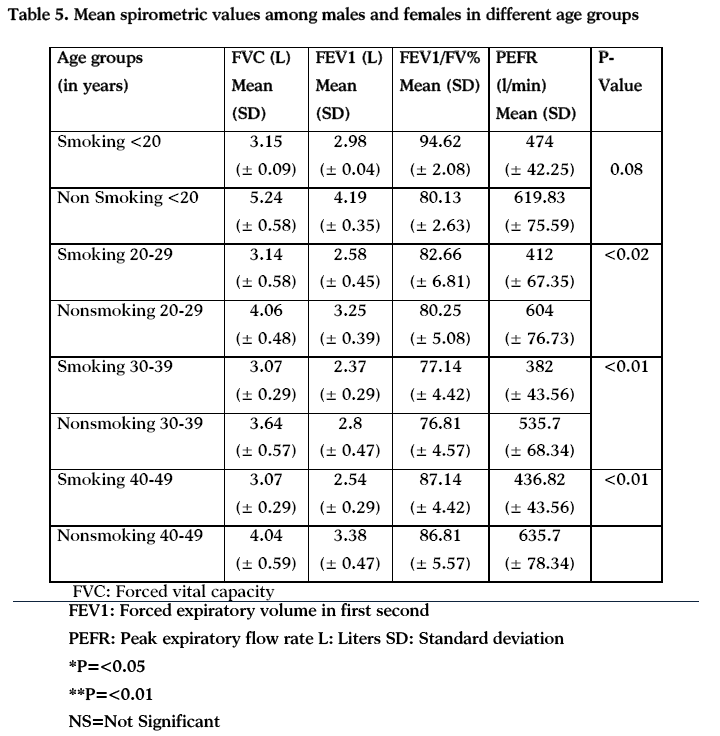
Table (5): shows that there is significant differences between mean spirometric values smoking and nonsmoking in age 20-30 years and 30-39and 40-49.
Discussion
Spirometry is a frequently performed lung function test and an important tool in medical surveillance examinations of pulmonary diseases. The interpretation of lung function relies on the comparison to reference values derived from a healthy population. The results of the current study have highlighted the importance of obtaining reference values and to develop prediction equations for these variables in our population. The mean values of FVC, FEV1, FEV1 / FVC % and PEFR in males and females were 4.38, 2.23, 75.60, 75.60 and 560 respectively, comparable to those of other local studies [11-18].
Although the mean values of the spirometry variables were found to be higher in males than females in all age groups, the difference in FVC was significantly higher in the younger age groups (more than 30 years). It was also observed that this difference in the mean values of FVC declined with subsequent increase in the age groups. This finding was in line with other international studies [19,20]. It was observed in the current study that the mean FVC and FEV1 declined in female. These changes were in affirmation with the observations made in other studies and can be associated to normal physiology. A study done by Dockery et al., [21] has found that the pre-adolescent girls have larger airways relative to lung size than the boys. Another study found that airways of women (20 -36 years of age) had 17% smaller diameter than the airways of mature men (23-48 years of age) [19]. These observations suggest the possibility that the geometry of female lungs may be different from male lungs. In a study on the morphometry of the lungs of 36 boys and 20 girls from 6 weeks to 14 years of age, boys tended to have larger lungs per unit of stature) [20]. That study further observed that although the number of alveoli per unit volume and area was identical in boys and girls, the total number of alveoli was larger in boys than girls resulting in larger lung volumes in boys. As a result of larger lung volume but proportionately smaller conducting airways at similar stature, boys are expected to have lower FEV1/FVC % at every age compared to girls of similar stature. Another variable which females consistently failed to exceed was PEFR. As PEFR is the most effort dependent pulmonary function, the difference may reflect gender differences in effort rather than in the function. However, more studies are required to explain the gender differences in the lung function.
Studies have found that measures of body weight and fat were inversely related to the spirometric variables. Adiposity, especially of chest and abdomen was considered to restrict the normal movements of chest and diaphragm) [23]. Age was found to be necessary independent variable for all spirometric parameters.
Conclusion
We conclude that mean FVC, FEV1 and PEFR were higher in nonsmoker in each age group. Lung function changes from adolescence to old age but it’s differing in males and females. BMI was not significantly associated with the most of spirometric values. In order to generalize these reference values, a larger study following the ATS criteria is needed. As the demographic and anthropometric characters change with the passage of time, a larger study following the criteria set by ATS is required for this purpose.
Recommendations
As previous studies recommended that university curricula must include information about smoking cessation [24,25]. The current study indicates that cigarette smoking is mainly a problem of male students; the smoking cessation support for youths in this country is urgently needed. The smoking epidemic is so huge that every effort is needed to launch an effective campaign to protect our people and maintain a good quality health life.
Acknowledgements
The researchers would like to thanks Al-Zarqa Private University for funding this research. Special thanks for the university students, staff and workers who participate in this study and for the university administration for facilitating the process of data collection.
3126
References
- Abbadi AA. Smoking as a public health challenge. J Med J 2010; 44 (4): 381- 38.
- Capro JD. Respiratory structure and function. In: Goldman L, Bennett JC, edi). Cecil text book of medicine. 21st ed. Philadelphia: Saunders, 2000: p.84-5.
- Lin FL, Kelso JM. Pulmonary function studies in a healthy Filipinos adult residing in United States. Journal of allergy and clinical immunology, 1999; 104(2):338–40.
- Golshan M, Nemat-Bakhsh M. Normal prediction equations of spirometric parameters in 799 healthy Iranianchildren and adolescents. Archives of Iranian medicine, 2000; 3(3):109–13.
- Ray CS. Sue Dy, Bray G, Hansen JE, WassermanK. Effects of obesity on respiratory function. Am Rev Respir Dis 1983; 128(3): 501–506.
- Sahebjami H. Dyspnea in obese healthy men. Chest 1998; 114: 1373–1377.
- Prasad BK, Sahay AP, Singh AK, Smoking women and their lung function tests. Kathmandu University Medical Journal, 2003;2(6): 142-144. 8. Azab M, Khabour OF, Alkaraki AK, Eissenberg T, Alzoubi KH, Primack BA. Water pipe tobacco smoking among university students in Jordan .Nicotine & Tobacco Research, 2010; 12(6):606-612.
- World Health Organisation. The Asia Pacific Perspective. Redefining obesity and its treatment. https://www.wpro.who.int/pdf/obesity_final.pdf 2000.
- Standardization of spirometry 1994 update. American Thoracic Society.Am J RespirCrit Care Med 1995; 152: 1107-36.
- Malik MA, Moss E, Lee WR. Prediction of ventilation capacity in male West Pakistani workers in United Kingdom. Thorax 1972; 27: 611-9.
- Williams DE, Miller RD, Taylor WF. Pulmonary function studies in healthy Pakistani adults. Thorax 1978; 33: 243-9.
- Hameed MA, Khan SA. Peak expiratory flow rate in healthy Pakistani adults. J Pak Med Assoc 1984; 34: 363-4.
- Ayub M, Zaidi SH, Burki NK. Spirometry and flow-volume curves in healthy, normal Pakistanis. Br J Dis Chest 1987; 81: 35-44.
- Hameed MA, Khan SA, Ahmed A. Pulmonary function studies in healthy Pakistani children. J Pak Med Assoc 1987; 37: 318-24.
- Hameed MA, Quraishi MS, Nuri MH, Alvi EA. Pulmonary function in healthy Pakistani adults at different altitudes. J Pak Med Assoc 1988; 38: 158-63.
- Siddiq M, Zaheerud Din, Beg Z. Spirometric values in normal Pakistani population. Pak Armed Forces Med J 1997; 47: 41-4.
- Nadeem MA, Raza SN, Malik MA. Ventilatory function of healthy, urban, nonsmoking, Pakistani young adults aged 18-24 years. Respir Med 1999; 93: 546-51.
- Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general U.S. population. Am J RespirCrit Care Med 1999; 159:179-87.
- Golshan M, Nematbakhsh M, Amra B, Crapo RO. Spirometric reference values in a large Middle Eastern population. EurRespir J, 2003; 22: 529-34.
- Dockery DW, Berkey CS, Ware JH, Speizer FF, Ferris BG Jr. Distribution of forced vital capacity and forced expiratory volume in one second in children 6 -11 years of age. Am Rev Respir Dis, 1983; 128: 405-12.
- Shishani K, Nawafleh, H. and SivarajanFroelicher, E. Jordanian Nurses' and Physicians' Learning Needs for Promoting Smoking Cessation. Progress in Cardiovascular Nursing, 2008; 23: 79–83.
- Shishani K, Nawafleh H, Jarrah H, SivarajanFroelicher E. Smoking practices among Jordanian health professionals: A study about the impediments to tobacco control in Jordan. European Journal of Cardiovascular Nursing, 2011; 10(4), 221-7.

