Keywords
Referral system; Patients; Level; Primary; Secondary; Tertiary; Health care; National document
Introduction
The National Coordinating Council with a national plan of patient referral system should be based on current health legislation, harmonization of unique standardized protocols with followup guidelines for patient referral system for all levels of health care, but this referral system of Patients should be regulated on the basis of guidelines and protocols approved by the Kosovo Ministry of Health. Lack of an effective program of the patient referral system related to setting, goals, mark possible sources of the referral system, creating a plan to achieve the identification of needs, forewarned resources are basic principles in a proper system of the referral system The management system of the referral system is a unified tool for health care providers to keep patients' referrals under control [1-5].
Purpose of the research
Its main purpose of this reflection system work is to improve the direction of communication between the three levels of health care with specialists and health care providers for the sick. The objective of this research is that health care professionals at three levels of health care should possess knowledge of the organization, knowledge of existing human resources, recognize the signs and symptoms of life-threatening disease, assess the condition of patients, situation, needs, risk and reference game in accordance with reference system standards [4-7].
Material and Methods
The applied methodology of this research is the goal and starting point for achieving the objectives of communication between the three levels of health care with specialists and health care providers for patients, based on legislation, standardized protocols and responsibilities at all levels of Health care, Country level, Applied methodology. The research material is taken from the collected guidelines and cases referred to by the primary and secondary level of health care for the period January-June 2018. The research is of retrospective, descriptive, qualitative type. In the research were obtained from 35,932 samples selected for research is only 1350 referral sheets. The sample selected was the diagnostic guide, the type of pathology, the municipality and the method of referral. Data collection methods and techniques. The research material is taken from the collected guidelines and cases referred to by the primary and secondary level of health care for the period January-June 2018. Sample description and data processing.
The sample examined 1350 referral sheets of the referred cases. The research was conducted on the basis of data obtained from the reference system of primary and secondary level at the national level, the research was analysed on the basis of statistical tests.
Work results
Out of the total number for the period January-June 2018, out of 35,932 referral sheets from the primary and secondary level, only 1350 referral sheets were selected for research. Samples selected from them intrinsically, surgically, orthopedically with trauma and surgery where the diseases and traumas have been researched, the reference levels from the regions, secondary.
Referral pathology from the primary and secondary level of health care to the Emergency Clinic. Types of pathologies above the disease dominate internist diseases 18835 cases or 52.41%, orthopedic and traumas 10752 cases or 29.94% and surgical 6345 cases or 17.65% (Table 1 and Figure 1).
Table 1 Types of pathologies.
| Types of pathologies |
Nr. of cases |
% |
| Internal diseases |
18835 |
52.41 |
| Orthopedic and trauma |
10752 |
29.94 |
| Surgery |
6345 |
17.65 |
| Total |
35.932 |
100 |
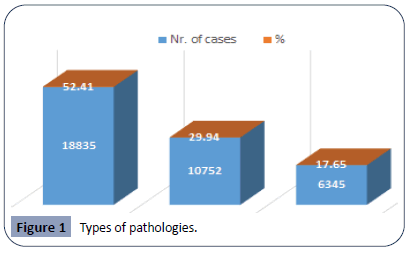
Figure 1: Types of pathologies.
Cases referred to by regions are led by Prishtina 23804 cases or 66.24%, Ferizaj with 4744 cases or 13.20%, Prizren 2854 cases or 7.74%, while other regions have fewer cases referred with special emphasis to the regional hospital of the part referred to only. 426 cases or 1.15%. This reference from the primary level of the Prishtina region is the lack of a city hospital (Table 2 and Figure 2).
Table 2 Referred from Regional Hospitals.
| Region |
Nr. of cases |
% |
| Prishtine |
23804 |
66.24 |
| Prizren |
2854 |
7.74 |
| Peja |
426 |
1.15 |
| Mitrovica |
3409 |
8.47 |
| Gjilani |
947 |
2.0 |
| Gjakova |
794 |
2.20 |
| Ferizaji |
4744 |
13.20 |
| Total |
35.932 |
100 |
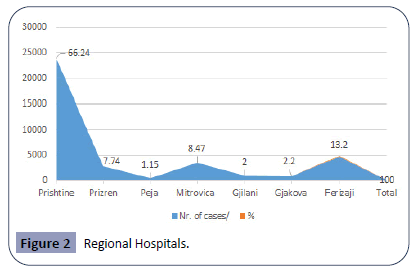
Figure 2: Regional Hospitals.
In Table 3 is present Selection of referral sheets from the primary and secondary level in the Emergency Clinic. Reference of cases from the primary level to the national level with 26479 cases or 73.69%, and secondary with 9253 or 26.31% (Table 4 and Figure 3).
Table 3 Referred from Regional Hospital and their municipalities.
| Region |
Nr. of cases |
Region |
Nr. of cases |
| Prishtine |
13460 |
Mitrovica |
881 |
| Fushe Kosove |
2854 |
Skenderaj |
889 |
| Podujeve |
3635 |
Zubin potok |
3 |
| Gllogoc |
2208 |
Leposaviq |
1 |
| Obiliq |
1600 |
Vushtri |
1635 |
| Gracanica |
47 |
Gjakova |
401 |
| Prizreni |
1205 |
Rahoveci |
170 |
| Suhareka |
206 |
Klina |
223 |
| Dragashi |
28 |
Gjilani |
597 |
| Malisheva |
369 |
Kamenica |
120 |
| Peja |
384 |
Vitia |
198 |
| Istog |
14 |
Partes |
10 |
| Deqan |
28 |
Ranilug |
22 |
| Ferizaji |
1249 |
|
| Kaqanik |
445 |
|
| Lipjani |
2484 |
|
| Shtimja |
540 |
|
| Shterpce |
26 |
|
Table 4 Referred from primary and secondary level.
| Referral case |
Nr. of cases |
% |
| Primary Health care level |
26479 |
73.69 |
| Secondary Health care level |
9253 |
26.31 |
| Total |
35932 |
100% |
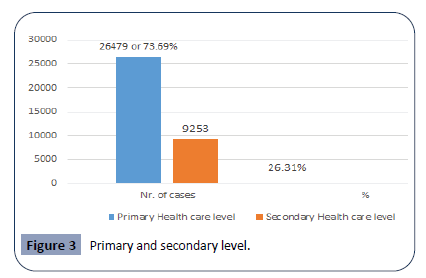
Figure 3: Primary and secondary level.
In Table 5 we show number of cases refereed from Primary health care level according to specializations in Emergency Clinic. Number of specialist consultations from a fields of gynegology is 2144 cases or 8.09%, consultations from Internal -medicine 12344 cases or 46.61%, surgery consultations 4543 cases or 17.15% and number of orthopedic consultations with trauma 7448 cases or 28.12%.
Table 5 Number of Cases Referred by Primary health care level in Emergency Clinic according to specializations.
| Referal |
Specialist consultations- Gynegology obs |
Specialist consultations in Internal medicine cardiology |
Specialist consultations in surgery |
Specialist consultations in orthopedics and trauma |
| Primary level |
2144 cases or 8.09% |
12344 cases or 46.61% |
4543 cases or 17.15% |
7448 cases or 28. 12% |
In Table 6 is present number of referrals cases from secondary level according to specializations in Emergency Clinic. Number of specialist consultations from a fields of gynecology are 121 cases or 1.30%, specialist consultations from Internal-medicinecardiology 5003 cases or 54.06%, specialist surgery consultations 1345 cases or 14.53%, and number of specialist orthopedic consultations with trauma 2785 cases or 30,09% .
Table 6 Number of Cases Referred by Secondary health care level in Emergency Clinic according to specializations.
| Referral |
Specialist consultations- Gynegology obs |
Specialist consultations in Internal medicine cardiology |
Specialist consultations in surgery |
Specialist consultations in orthopedics and trauma |
| Secondary level |
121 cases or 1.30% |
5003 cases or 54.06% |
1345 cases or 14.53% |
2785 cases or 30,09% |
Discussion
Based on the WHO document, Management of health facilities: referral systems, the continuous increase of the capacities of the health care staff, education and training of doctors, nurses at the level of primary and secondary health care. Referring to the work of the author Prudhomme a Health Records Review of Outpatient Referrals from the Emergency Department. 2019, is based on significant differences both in the waiting time and in the reliability of outpatient referrals in emergency services indicate high performance and that common referral processes. The three-level referral health care system in Kosovo is chaotic, disorganized, without guidelines, protocols of the referral system; the Ministry of Health of Kosovo must take into account all the details to regulate the normative acts of the referral system at the national level [1-10].
Regional hospitals keep their cases in their institutions for a few hours or a few days and with a lack of instruction or epicrisis by not using professional medical resources, and instead of exhausting all their resources and in the absence of specialties (Neurosurgeon, surgeon thoracic, urologist, vascular, cardiac surgeon, invasive cardiologist) with recommendation and permission can be sent for further treatment, or some of them are sent unprocessed to the Tertiary Care [1,8,10].
The health care referral system is a written order from the primary care physician that the patient can be seen by a specialist or receives certain medical services. Referral system procedures are a procedure used to resolve issues such as medical concerns over patient safety by harmonizing their health with a recommendation for a harmonized position throughout the EU. The process of generating a clinical referral for a patient, and the result of transferring information from the primary care physician to the specialist and again, are key components in the fight to provide less costly and more effective clinical care [2,4,11].
Primary and secondary institutions should use their professional capacities, and if the patient or injured person who is treated in primary institutions or in a regional hospital and needs more specialized diagnosis, treatment and examination, should be equipped with an epicrisis and sent to tertiary care, after consultation signed by the treating physician. the family doctor, the head of the unit or the director of the hospital or the person authorized by him [12].
The reasoned decision to refer the patient from the primary, secondary institution to a more specialized hospital to be documented in the patient's personal health card. All cases referred for treatment or examination to another hospital should be documented in a separate register and stored in the archive of the sending hospital. The patient who is treated in a regional hospital and needs more specialized diagnosis, treatment and examinations, to be equipped with an epicrisis and to be sent to the UCCK (University Clinical Center of Kosovo) after a consultation signed by the treating physician. The head of the unit and the director of the hospital or the person authorized by him. The reasoned decision to refer the patient to a more specialized hospital to be documented in the personal health card of the patient [1,8,10].
All cases referred for treatment or examination to another hospital should be documented in a separate register and stored in the archive of the sending hospital. The directorate of the institution displays in visible places the way of organizing the consultation (place, day, and schedule) and the fees for each consultation or medical examination, for the uninsured or uninsured persons with the above mentioned documentation [7].
All cases defined as medical emergencies referring to hospital treatment by the outpatient service must have a recommendation from the general practitioner and the family, while those sent by the regional hospital to the UCCK must possess the accompanying epicrisis signed and stamped by the physician. Guardian and head of the relevant unit. Extraordinary medical emergencies are excluded from this rule1, when the patient goes directly to the regional hospital or UCCK [13].
Defects of some reference sheets from the primary and secondary level, it is clear that the responsibility, obligations and obligations that belong to them, or the recognition or non-recognition of the signs and acute symptoms of diseases or injuries, or the use of professional diagnostic, laboratory capacities, lack data or written only general data, does not specify the length of stay of patients are issues that need to be discussed in solving this problem [2,7].
The Ministry of Health of Kosovo may regulate this system on the basis of instructions and protocols approved by the Ministry of Health of Kosovo by dividing the roles and responsibilities of primary, secondary and tertiary level, based on listing diseases, injuries and poisoning because the primary level hold the primacy 73.69% while from regional hospitals 26.31%. Cases reflected in the solvent level. Emerging services account for only 20% of the total number of cases [3].
All care professionals involved should be subjected to education, training on how to refer to the system in which cases should be sent from the first level to tertiary care and to understand the laws governing the health system of Kosovo and how to respond. Effectively referral system. The mechanisms of the referral system function at different national, regional and municipal levels based on national laws and policies and work on the basis of efficient lines of communication by creating clear and simple steps and procedures described. The functioning of the mechanisms of the referral system is based on legislation, standardized protocols which define the roles and responsibilities at all levels of health care [5,9].
The decision-making of the referral system is a clinical decision made by primary and secondary level physicians with a referral indication, whether referral is necessary or not, coordinating activities with the tertiary level. Preliminary results show that the new computer-based referral process is faster to use than conventional methods. If professional resources are depleted or in the absence of specialties from internist and surgical branches, etc. and a referral system is used as a tool to facilitate the flow of referrals of patients among health care providers by improving the results of medical care and treatment and reducing costs through optimal use of medical services. Against the penalties imposed on this order. The penalized person can appeal to the Authority that imposes the penalty on the Directorate of Health and Social Welfare of the municipality (Primary doctor), the Law on Inspectorate [6,11].
Emergency medical care law. The Law on Health Insurance and other laws that regulate the health system of Kosovo, within 5 days from the day of receiving the notification. For the sanction imposed on him. The relevant authority shall respond within 10 days from the day of filing the complaint. Against the decision of the Authority that imposes the penalty, the person can appeal to the central institutions (M of health and KHIS) within 5 days from receiving the answer. The relevant institution responds within 30 days. In cases of repeated violations, administrative measures will be applied to the head of the health institution according to the provisions of the Labor Code and the Collective Agreement, until dismissal [4,12].
The HUCSK Directorate, the Directorates of Regional Hospitals, the Directorate of Health and Social Welfare (Primary Physician) are in charge of the implementation of this order. To monitor this order in the future, the Institute of Health Insurance IKSHP, the Directorate of Regional Hospitals at the Ministry of Health, and the Directorate of Audit in the Ministry of Health should be charged. This ordinance should be functionalized as a recommendation and should later be accepted as a mandatory guideline signed by the Minister of Health of Kosovo, which should be based on; Law on Health, Law on Health Inspectorate 2006/02-L38.
Law on Public Health 2007/02-L78, Law on Emergency Health Care), Labor Law, and the Collective Labor Agreement, as amended, as well as other acts in force, regarding the rules for the treatment of patients referred for visits and medical consultation with a specialist or UCCK, in order to improve the quality of medical care.
Serving On the functioning of the c referral system of patient’s health services. Given the obstacles to the referral system, improvements are necessary and necessary to promote the quality of health care at three levels of health care as such changes require coordination between the three levels of the referral system, strengthening the public sector of the referral system, raising public awareness of the referral system and preventing self-referral [1,6,9,13].
Conclusion
The family doctor at the primary level and the regional hospitals. The regional hospitals remain as a point of discussion in the patient referral system, despite the spatial capacities at the primary level, they keep the primacy 73.69% while from the regional hospitals 26.31%.
Relating to case reports from the primary level, there is no professional justification because the cases referred to over 80% are of non-emergency nature (minor injuries, chronic cases, unconvincing diagnoses, raw cases not using professional medical capacities and consultations within, where the patient's last name is marked, the referral diagnosis without registration of vital signs and the actions they have in their institution.
Whereas the regional hospitals their cases stay for a few days in the hospitals with a lack of instruction or epicrisis by not using the resources within the hospital. Regional hospitals should exhaust all their resources and in the absence of specialties (Neurosurgeon, Thoracic Surgeon, Urologist, Vascular, Cardiac Surgeon and Invasive Cardiologist) with recommendation and leaflet were sent for further treatment at UCCK.
Some municipalities of Kosovo little ones like Rahovec, Malisheva, Klina, Skenderaj must not be sent to the nearest hospitals, but they must be sent to the UCCK immediately.
Creating referral system forms should be with patient compliance details and proper communication between health care levels. Advancement, strengthening and regionalization of health care services and implementation at three levels of health care.
The Ministry of Health of Kosovo should regulate the referral system in Kosovo, which is currently disorganized chaotic, and the Ministry of Health should draft a national document of the referral system for patients at the health level by educating and training health care professionals at the entire level, Health care.
The National Coordinating Council should modify a national plan of the patient referral system based on current health legislation, harmonization of unique standardized protocols with followup guidelines for patient referral systems for all levels of health care, the Ministry said. Effective programs of the patient referral system related to setting, goals, mark the possible sources of the referral system, create a plan to achieve the identification of needs, warned resources are basic principles in a proper system of reference. The Ministry of Health must have a national document of the system of referral of patients at the health level, which first of all health care professionals are educated, trained on the way of the referral system, which cases should be sent from the primary, secondary level and tertiary.
Disclosure
The authors declared no conflict of interest. No funding was received for this study.
Acknowledgement
We would like to thank medical staff of Emergency Clinic of the University Clinical Center of Kosovo.
28367
References
- Elo S, Kyngas H (2008) The qualitative content analysis process. J Adv Nurs 62: 107-115.
- Bossyns P, van Lerberghe W (2004) The weakest link: competence and prestige as constraints to referral by isolated nurses in rural Niger. Human Resources for Health 2.
- A computer-based outpatient clinical referral system. International Journal of Medical Informatics 55: 149-158.
- Cervantes K, Salgado R, Choi M, Kalter H (2003) Rapid Assessment of Referral Care Systems: A Guide for Program Managers.
- Alleyne G, Claeson M, Evans DB, Jha P, Mills A, et al. (2006) Disease Control priorities in Developing Countries. A co publication of Oxford University Press and The World Bank.
- Saunders D, Kravitz J, Lewin S, McKee M (1998) Zimbabwe’s hospital referral system: does it work? Health Policy Plan 13: 359-370.
- Stuart L, Harkins J, Wigley M (2005) Establishing Referral Networks for Comprehensive HIV Care in Low-Resource Settings. The HRH Global Resource Center.
- Measure Evaluation (2013) Referral systems assessment and monitoring toolkit. USAID.
- (2019) Archives of Emergency Clinic University Clinical Center of Kosovo.
- Ross J (2008) Rural Nursing: Aspects of Practice. New York, NY: Rural Health Opportunities.
- Carty RM, Al-Zayyer W, Arietti LL, Lester AS (2004) International rural health needs and services research: a nursing and midwifery response. J Prof Nurs 20: 251-259
- Harvey DJ (2010) The Contribution of Qualitative Methodologies to Rural Health Research: an Analysis of the Development of a Study of the Health and Well-Being of Women in Remote Areas. International Journal of Qualitative Methods.

