Keywords
Teenage pregnancy, adolescent pregnancy, teenage childbearing, risk factors
Introduction
The negative obstetric and foetal outcomes as well as social consequences associated with teenage pregnancies are well documented globally and regionally [1-3]. Preventing teenage pregnancy is important in achieving the millennium development goals of maternal and child survival [4].
A pregnancy occurring in a young woman who has not reached her 20th birthday is considered as a teenage pregnancy. This definition is applicable irrespective of the legal status of the marriage of the woman or legal age to consider an individual as adult [5]. A couple whose marriage is registered by the Registrar of marriage is considered as a legal marriage.
Teenage pregnancies is a global phenomenon. The pregnancy rate among teenagers in USA was 67.8 pregnancies per 1,000 women aged 15–19 in 2008.6 Among the countries in the western Europe, the United Kingdom (UK) has the highest teenage conception and abortion rates.7 The rate of conception rate among those under 18 years in the UK was 40.5 per 1000 in 2008. This is five times higher than the rate in Netherlands, more than twice the rate in Germany and twice the rate in France [8].
The reported teenage pregnancy rates in South Asian countries Bangladesh, Nepal and India are 35%, 21% and 21%, respectively [9]. A possible explanation for this is the fact that in these countries arranged teenage marriages are common and culturally; these teengirls are expected to be pregnant within one year of marriage. Teenage pregnancy rate in Sri Lanka is much lower than the rates in these South Asian countries. Reproductive health information database of Family Health Bureau of the Ministry of Health, Sri Lanka, indicate that 6.5% of the total pregnancies registered during the year 2010 were teenage pregnancies [10]. The Demographic and Health Survey, Sri Lanka, 2006/07 revealed that 6.4% of women had begun childbearing when they were teens [11].
In view of the range of negative medical and social outcomes, it is pertinent to launch interventions to avoid teenage pregnancies. Identifying the risk factors that influence the occurrence of teenage pregnancies is the basis on which effective preventive programmes should be developed.
Residing in disorganized/dangerous neighbourhoods and in a family with lower socio-economic status, low educational attainment, living with a single parent, having older sexually active siblings or pregnant/parenting teenage sisters, and being a victim of sexual abuse, poor parent/child closeness, poor parental supervision or regulation of children's activities have been found to be factors elevating the risk of teenage pregnancy in USA [12]. Socioeconomic disadvantage, disrupted family structure and limited education, risky sexual behaviours such as early sexual initiation, increasing number of partners and non-use of contraceptives, alcohol, drug or tobacco use were the factors associated with teenage pregnancies in European Union countries [13]. The risk factors identified for teenage pregnancy in South Asian countries of Bangladesh, India and Nepal include low socio-economic background, low educational attainment, disrupted family structure and poor sexual health practices [9].
Two previous studies in Sri Lanka conducted in hospital settings with older pregnant women as the comparison group have mainly focused on assessing adverse outcomes of the pregnancies per se [14,15] However, they have reported that teenage groups were poorer and less educated than the comparison group. A comprehensive assessment of risk factors for a teenager to become pregnant in comparison to non-pregnant groups has not been reported in Sri Lanka, to date.
Aim
This study aimed at identifying the risk factors of teenage pregnancies in a Sri Lankan setting.
Material and methods
This study was carried out in three districts of Sri Lanka, Anuradhapura, Batticaloa and Colombo. These districts were purposively selected, based on the information that they reported high percentages of teenage pregnancies [10]. Within each district, three basic health administrative areas (Medical Officer of Health (MOH) divisions) with high rates of teenage pregnancies were included in the study.
Study population comprised all pregnant females resident in the selected MOH areas, who had not completed their 20th year at the time they became pregnant and were registered with the Public Health Midwife (PHM) for antenatal care. The proportion of pregnant women registering with PHM in the study area is reported to be over 90% [10]. The comparison group comprised of age matched non-pregnant females residing in the same MOH area. Study units were identified from the registers of the PHM over a period of three months.
For each pregnant teenager, a non-pregnant female was identified from the neighbourhood. Age of the teenagers was verified using the identification documents. A total of 93% of the study and comparison units were able to produce such document at the time of recruitment into the study. The age of conception was verified to be prior to the 20th birthday by cross checking the information on the period of amenorrhea on clinic records with the age. A total of 510 pregnant teenagers and 508 non-pregnant teenagers were included in the analysis. Post-hoc power analysis applied to the variable of education level of the two groups revealed that this sample size was adequate to provide a power of over 90% to detect a difference.
Data were collected using a structured interviewer administered questionnaire. A thorough literature review on research related to risk factors for teenage pregnancy was performed prior to the development of the questionnaire to identify risk factors that have been identified by other researchers, especially by those in the Asian countries. Potential risk factors for the local setting were identified using the information gathered. Risk factors for teenage pregnancy were grouped into socio-demographic and other personal characteristics of the teenagers, characteristics of the spouses /partners, and parents, family interactions, teacher and peer support, knowledge related to pregnancy, knowledge on contraceptives and opinion on contraceptive services. Thereafter, questions were formulated to gather information on the risk factors and a panel of experts in the field of maternal and child health and reproductive health were invited to a round table discussion to assess the validity of the questions. The panel assessed whether all potential risk factors have been adequately represented, assessing the content validity. At this meeting, initially the experts perused the questions individually and the issues they had were later discussed as a group till a consensus was arrived at.
In addition to the questions on risk factors, the questionnaire for the pregnant teenagers contained a few additional questions related to details of the pregnancy such as, parity, planning of the current pregnancy, reasons for getting pregnant in the cases of a planned pregnancies and the use of contraceptives in the cases of unplanned pregnancies. The panel of experts assessed the content validity of these questions as well.
The validated questionnaires were then translated into two local languages Sinhalese and Tamil by two bilingual specialists. These were back translated to English by another two bilingual specialists to confirm the accuracy of the translation. The translated versions of the questionnaires were pre-tested among two groups of 10 pregnant teenagers and 10 non-pregnant teenagers resident in an MOH area outside the study areas. A few questions required re-wording and they were tested again for clarity and appropriate modifications were made.
The reliability of the questionnaires was assessed using test-retest method. Following one week after data collection, selected important questions of the questionnaire with responses in categorical form was re-administered to 20 pregnant teenagers and 20 non-pregnant teenagers from each of the three MOH area. Test-retest reliabilities of these categorical variables were assessed using Cohen’s kappa and the minimum Cohen’s kappa coefficient was 0.76 for the variables included.
Data were collected by trained interviewers who were fluent in the relevant mother tongue of the respondent.
Informed verbal consent was obtained from the teenagers as well as the parents in the case of all respondents who were living with their parents and where the teenagers were living on their own, consent was obtained from the teenagers themselves. Those who were above the age of 20 years provided informed verbal consent personally. Interviews were conducted at settings within the community or at homes of the participants based on their choice. All measures were taken to ensure privacy of participants and confidentiality of the information.
Ethics Review Committee of the Faculty of Medicine, University of Colombo approved the study protocol. The study was conducted from December 2010 to April 2011.
Data were analyzed using the Statistical Package for the Social Sciences (SPSS version 16). A variable on overall knowledge related to disadvantages of teenage pregnancy was created by scoring the responses to the two questions related to teenagers not being physically and mentally prepared for a pregnancy. Those who responded accurately for both questions were categorised as having ‘good’ overall knowledge on disadvantages of teenage pregnancy while those who answered only one or both questions inaccurately were categorised as having ‘poor’ knowledge on disadvantages of teenage pregnancy. In the univariate analysis, socio-demographic and other characteristics of the teenagers, factors related to marriage/cohabiting status, perceived self-confidence in decision making, characteristics of spouse/partner and parents, perceived support from family, support from peers and school teachers in resolving problems, knowledge on reproductive health related to pregnancy and knowledge regarding contraceptives and opinion regarding contraceptive services were assessed for association with teenage pregnancy by calculating the Odds Ratios (OR) and 95% confidence intervals (CI). Statistical significance for the association was tested using the Chi-square test.
Adjusted risk factors for teenage pregnancy were evaluated by using multiple logistic regression modelling. All factors that showed a significance level of p<0.05 in the univariate analysis were entered in the model and non- significant factors (p>0.05) were eliminated in a step-wise manner. Results are expressed in terms of adjusted ORs and 95% CIs.
Results
Among the pregnant teenagers, 9.8% (n=50) were 16 years or less, 47.1% (n=240) were within 17- 18 years while 39% (n=199) were 19 years and 4.1% (n=21) were 20 years old at the time of survey. The majority were Sinhalese (n=269, 52.7%) with the proportion of Tamils and Muslims being 30% (n=154) and 17.3% (n=87) respectively. Of the group, only 1% (n=5) have had no schooling. Only 9.6% (n=49) had studied beyond General Certificate of Education- Ordinary Level (GCE O/L). Approximately one fourth (n=133, 26.1%) had been engaged in paid work during the previous year with 12 (9%) among them, being engaged in paid work at the time of study.
Of the pregnant teenagers 41(8%) indicated that this was their second pregnancy with 18 (43.9%) of them with a living child. None reported more than one previous pregnancy.
Among the study group, 59.6% (n=304) reported that the pregnancy was planned with 40.4% (n=206) saying that it was unplanned. The commonest reason given for a planned pregnancy was ‘husband’s wish to have a baby’ (n=243, 79.9%). Of the 206 unplanned pregnancies, 31.1% (n=64) used a contraceptive method, a majority using oral contraceptives (n=38, 59.4%).
Of non-pregnant comparison group, 30.5% (n=155) were married or co-habiting at the time of survey.
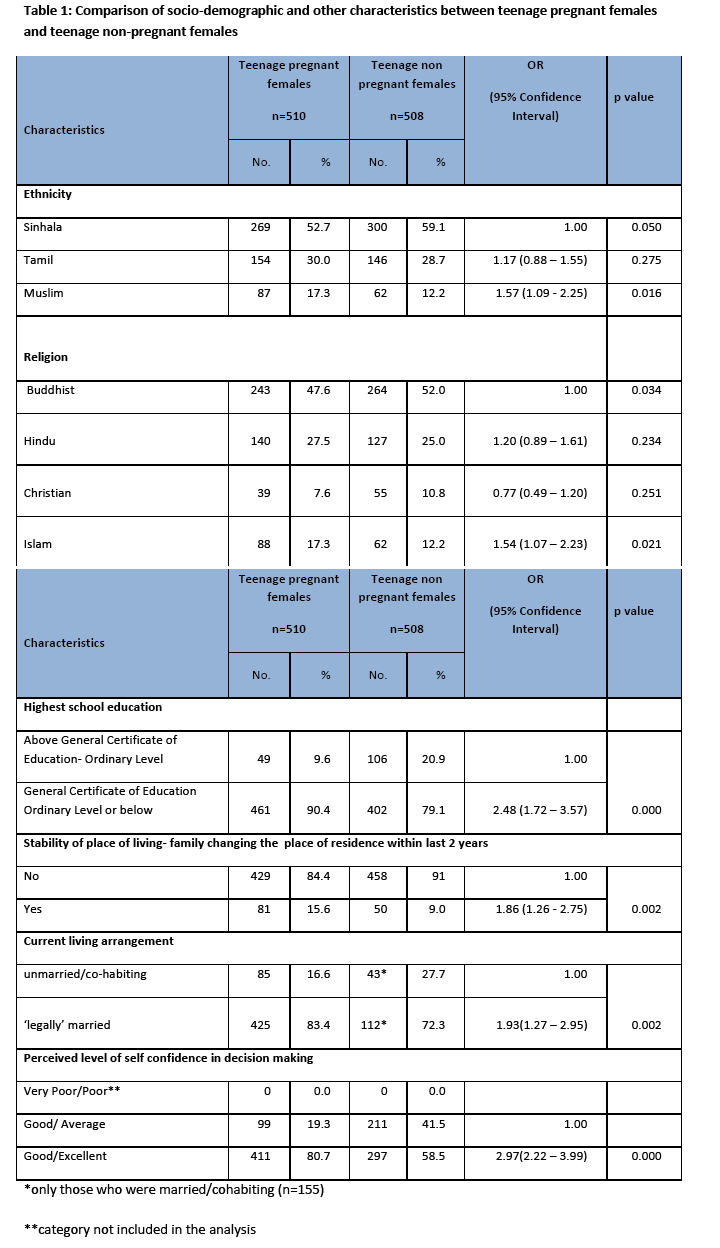
In the univariate analyses, level of education, up to GCE O/L or below (OR=2.48, 95%CI 1.72-3.57, p<0.001), instability of the place of living as indicated by having changed their residence within last two years (OR=1.86, 95%CI 1.26-2.75, p=0.002), belonging to the ethnic group Muslim(OR=1.57, 95%CI 1.09-2.25, p=0.016) and practising Islam .religion (OR=1.54, 95%CI 1.07– 2.23, p=0.021), emerged as risk factors (Table 1). Being ‘legally’ married as opposed to co-habiting with the spouse/partner was also found to be a risk factor for a teenage pregnancy (OR=1.93, 95% CI 1.27-2.95, p=0.002). Those who perceived their level of self confidence in decision making to be ‘excellent’ were at a higher risk for teenage pregnancy (OR=2.97, 95% CI 2.22-3.99, p<0.001).
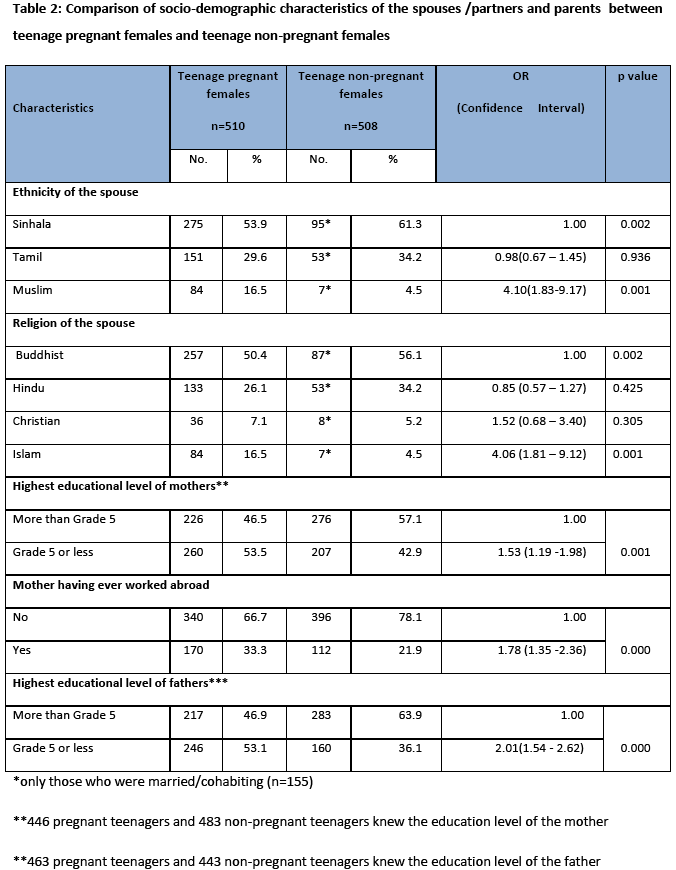
As shown in Table 2 ethnic and religious affiliations of the spouse also showed higher odds for having a teenage pregnancy if the spouse was a Muslim (OR=4.10, 95%CI 1.83-9.17, p=0.001) and practiced Islam (OR=4.06, 95%CI 1.81–9.12, p=0.001).Socio-demographic factors related to the mother and father of respondents showed that the mother having a level of education of grade five or less (OR=1.53, 95% CI 1.19-1.97, p<0.001), having ‘ever worked abroad’ (OR=1.78, 95% CI 1.35-2.36, p<0.001), and father having an education up to grade five or less (OR=2.01, 95% CI 1.54-2.61, p<0.001) were risk factors for a teenage pregnancy. Parental income, age at marriage or age at first pregnancy of mother or sisters were assessed but were not found to be risk factors for teenage pregnancy.
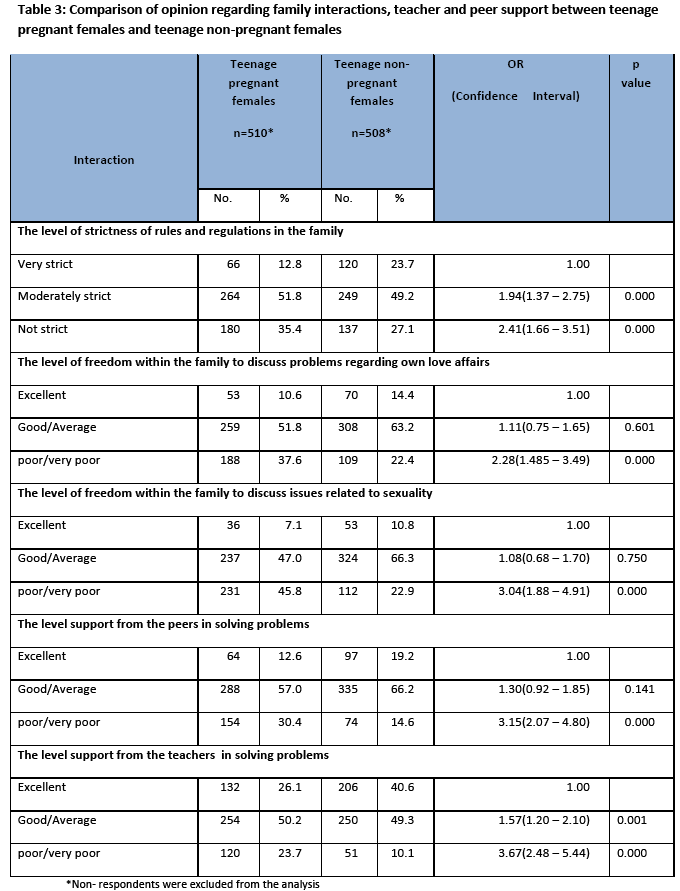
The risk of teenage pregnancy was high when the level of strictness of rules and regulations in the family was perceived as ‘not strict’ (OR=2.41, 95% CI 1.66–3.51, p<0.001) and when the level of freedom within the family to discuss problems regarding love affairs (OR=2.28, 95% CI 1.49–3.49), p<0.001); the level of freedom within the family to discuss issues related to sexuality (OR=3.04, 95% CI 1.88 – 4.91, p<0.001) were perceived by the teenager as poor or very poor (Table 3). Risk of teenage pregnancy was also high when the level of support from teachers (OR=3.15, 95% CI 2.07–4.80, p<0.001) and peers (OR=3.67, 95% CI 2.48–5.44, p<0.001), in solving problems was perceived as poor or very poor.
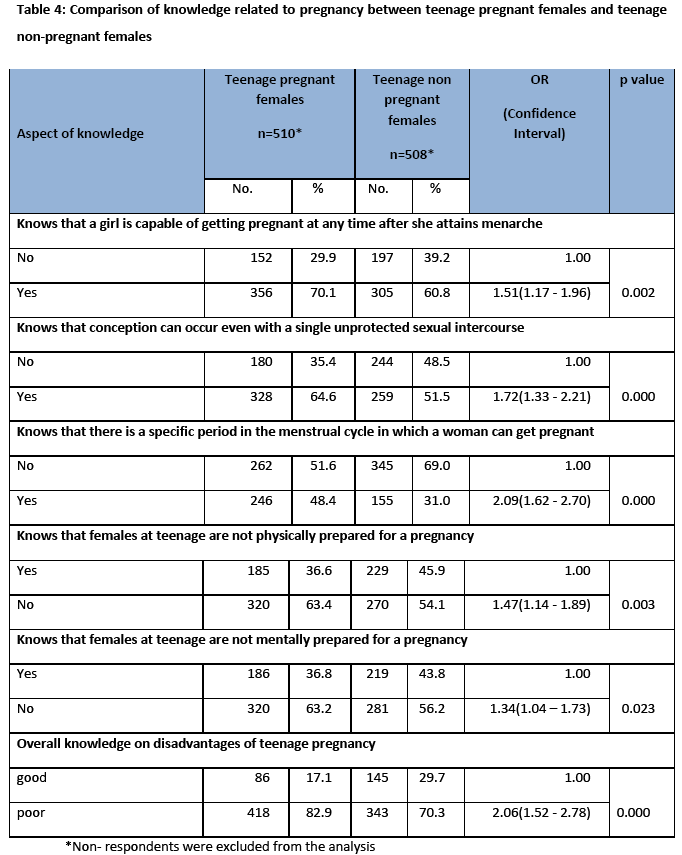
Pregnant teenagers had significantly higher level of knowledge on the following aspects: ‘a girl is capable of getting pregnant at any time after she attains menarche’ (OR=1.51, 95% CI 1.17-1.96, p=0.002); ‘conception can occur even with a single unprotected sexual intercourse’ (OR=1.72, 95% CI 1.33-2.21, p<0.001); ‘there is a specific period in the menstrual cycle in which a woman can get pregnant’ (OR=2.09, 95% CI 1.62–2.70, p<0.001). However, their level of knowledge on disadvantages of teenage pregnancy was significantly lower as revealed by responses to the statements ‘teenage pregnant are not physically prepared for a pregnancy’ (OR=1.47, 95% CI 1.14–1.89, p=0.003) and ‘females at teenage are not mentally prepared for a pregnancy’ (OR=1.34, 95% CI 1.04–1.73, p=0.023)). The knowledge related to association between teenage pregnancies and low birth weight of the babies and birth complications were similar among both groups.
Based on all questions related to disadvantages of a teenage pregnancy, teenagers were categorized as having a ‘good’ level of knowledge if she gives correct responses to all four questions. Overall, having poor knowledge on the disadvantages of teenage pregnancies was associated with a higher risk of teenage pregnancy (OR=2.06, 95% CI 1.52 - 2.78, p<0.001) (Table 4).
Assessing the knowledge on contraception, a significantly higher proportion of pregnant teenagers were able to name at least four modern contraceptive methods (OR=1.50, 95% CI 1.00–2.25, p=0.048) compared to the non-pregnant teenagers. A significantly higher proportion of pregnant teenagers disagreed that there should be special health services for young people to obtain contraceptives (OR=1.51, 95%CI 1.12 - 2.12, p =0.008) (Table 5).
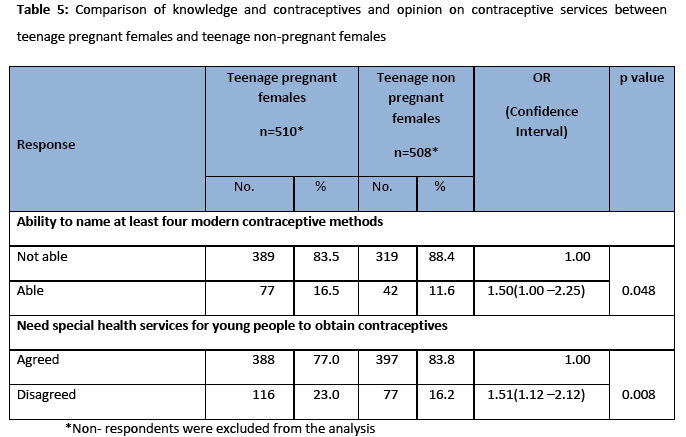
The study also compared attitudes of pregnant teenagers towards use of contraceptives. The responses to the attitudinal statements were similar among both groups such as ‘the number of children born to a family should not be limited by artificial methods’, ‘using family planning methods can harm the future pregnancies’, ‘using condoms reduces sexual pleasure’, ‘contraceptive methods are not suitable for young females’ and ‘practicing family planning is a sin’ etc.
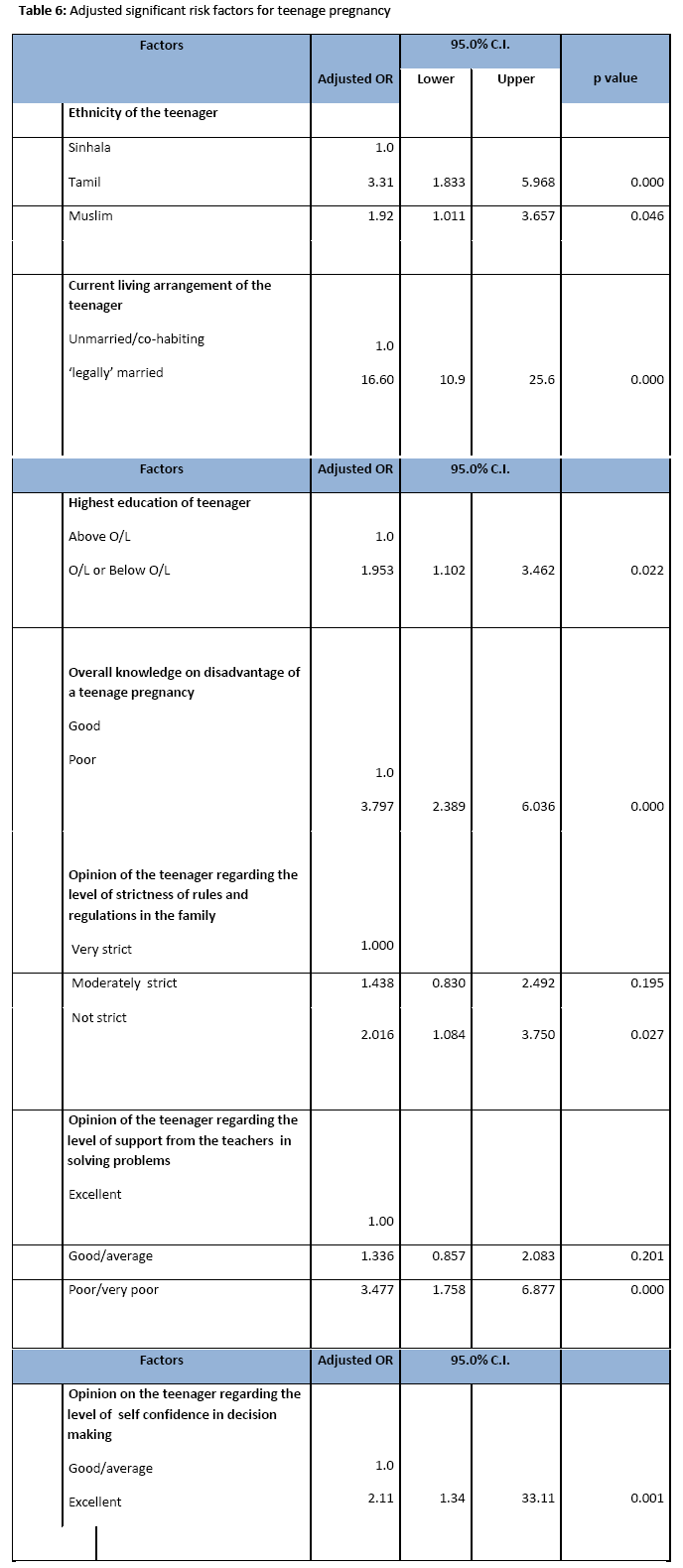
Adjusted risk factors for teenage pregnancy were assessed using a multivariate logistic regression model and the significant risk factors are shown in Table 6. Belonging to the ethnic groups Tamil (OR=3.31, 95% CI 1.83–5.96, p<0.001) or Muslim (OR=1.92, 95% CI 1.01–3.66, p=0.04), being ‘legally married’ (OR=16.6, 95% CI 10.9–25.6, p<0.001), the highest educational level being O/L or below O/L (OR=1.95, 95% CI 1.1–3.46, p=0.022), having a poor overall knowledge on disadvantage of a teenage pregnancy (OR=3.79, 95% CI 2.39–6.04, p<0.001), perception of teenager that the level of strictness of rules and regulations in the family as ‘not strict’ (OR=2.01, 95% CI 1.08–3.75, p=0.027), perception of the teenager that the level of support from the teachers in solving problems is poor/very poor (OR=3.47, 95% CI 1.76–6.88, p<0.001) and perception that her level of self confidence in decision making is excellent (OR=2.11, 95% CI 1.34–33.11, p=0.001) were the risk factors for teenage pregnancy as identified by the adjusted ORs.
Discussion
Conducting a community based study enabled inclusion of a comparison group matched for age and area of residence. Thus, factors identified can be considered to be unaffected by the variations due to socio-cultural factors specific to the area of residence.
In the present study, the age pattern revealed a low proportion of very young pregnant teenagers with 9.8% being 16 years or less. The corresponding proportion was 27.5% in a hospital based study in southern part of Sri Lanka reported in 2005.14 A mean age of marriage of 15.9 years has been reported from rural Nepal with most ending up in early teenage pregnancies [16]. In the USA 15 to 17 year olds comprised approximately 25% of teenage pregnancies [17] while 18% of conceptions among teens below 18 years in the UK were to girls aged under 16 years [18].
The proportion of unplanned pregnancies was 40.4% in the present study. The study from Sri Lanka in 2005 reported unplanned pregnancies in 54% of young teenagers (< 16 years) and in 23% of older teenagers (>16 years) [14]. Nepal reported higher figures of 47% unplanned and 34% undesired pregnancies [19]. Nepalese pregnant teenagers being much younger to Sri Lankan pregnant teenagers would have contributed to the differences. The studies in the UK20 and in USA21 has focused on the rates of teenage conceptions that end up as legal abortions which has been assessed to be approximately 50%.
Of those who had not planned the pregnancy, 68.9% had not been on any contraceptive method indicating an unmet need for services, which is further highlighted by the fact that a significantly higher proportion of pregnant teenagers indicated the need for special health services for young people to obtain contraceptives. Furthermore, of those who were practicing a contraceptive method, 59.4% had conceived while on oral contraceptive pills indicating method failure.
The commonest reason (79.9%) to become pregnant among those who planned the pregnancy was ‘husband’s wish to have a baby’. Nepal reported that 51% claimed that the authority over conception remains with their husband [22]. An imbalance of gender roles within a relationship is a common phenomena in South Asian countries. The fact that a significantly higher proportion of pregnant teenagers rated themselves as ‘excellent’ in decision making but have indicated a husband’s decision as a reason to become pregnant, indicate influence of gender imbalances in this situation forcing teenagers to give birth before they are emotionally or physically ready.
A relatively lower attainment of educational status which was found to be a risk factor for teenage pregnancy in the present study is well documented as a risk factor for teenage pregnancy in USA, European countries and in South Asian countries [9,12,13,16,19,22]. Two previous hospital based studies in Sri Lanka also reported that pregnant teenagers are comparatively less educated (p<0.01) [14,15]. However, it should be noted that in the present study, among those grouped as belonging to a lower education level, a majority (90.2%) have had six to ten years of formal school education. Only 10.6% had no formal school education or only primary education. This is in contrast to Sharma et al, [19] in 2001 who showed that among Nepalese teenage mothers 19% had not studied beyond primary school education, the difference being due to the generally high level of school participation by females in Sri Lanka.
Low socio-economic status is another risk factor for teenage pregnancy which is a consistent finding in developed countries and in South Asian countries [9,12,13,16,19,22] including the studies in Sri Lanka [14,15]. The present study utilised a comparison group matched for the area of the residence. It is likely that the socioeconomic status was also made similar in the two groups making it less likely to be highlighted as a risk factor.
A study in Nepal reported that Hindu teenagers are more likely to become pregnant (p<0.001) than Buddhist teenagers [19]. The present study reported that Islam teenagers are more likely to become pregnant compared to Buddhist tor Hindu teenagers. It should be noted that there is a scarcity of literature on teenage pregnancy risk factors from South Asian countries like Pakistan and Maldives with high proportions of populations following Islam religion.
Legal age of marriage in Sri Lanka is 18 years. In the present study 83.4% claimed that they were ‘legally married’. However, age distribution showed that 50% of pregnant teenagers are under the legal age of marriage even at the time of survey. In Sri Lanka when underage couples request their marriage to be registered, the marriage registrars issue a document to notifying them the earliest date that they can get married (the date the couple reach the legal age of marriage). It was found that this document was regarded as a ‘legal marriage certificate’ by teenagers. In the present study, those who reported being ‘legally married’ were at a higher risk of teenage pregnancy may be because they felt secure in their relationships.
The reported studies from South Asia had assessed only knowledge on contraceptives among the teenagers [9,16,22] They have presumed that teenage girls are unaware of the process of conception and dangers of unplanned pregnancy before the onset of pregnancy. The present study explored a wider scope of knowledge and found that pregnant teenagers had significantly higher knowledge regarding process of conception compared to non- pregnant teenagers. This has to be interpreted carefully as pregnant teenagers may have gained this knowledge following conception. In contrast to this, knowledge regarding disadvantages of teenage pregnancy was significantly lower than the comparison group. This finding make the authors of present study agree with other South Asian researchers [9,16,22] that teenage mothers would have delayed the index pregnancy if they had known its consequences beforehand.
Low level of strictness of rules and regulations in the family which can be considered as indicating poor parental supervision was a risk factor for teenage pregnancy. This indicates the felt need of parental supervision by the teenager. This situation may be related to the reported proportion of 33% mothers ‘ever worked abroad’ usually as housemaids in countries of the Middle East which is commonly seen among low income families in Sri Lanka. Poor parental supervision was also a risk factor for teenage pregnancies in USA [12]. The need of adult support for teenagers is further highlighted by the fact that a significantly higher proportion of pregnant teenagers were of the opinion that level of support from the teachers in solving problems was low.
The limitations of this study include selection of a purposive sample and the cross-sectional nature of data for assessment of risk factors. However, the study followed a rigorous methodology and revealed plausible associations which would have implications for policy and practice to prevent teenage pregnancies.
Conclusion/Recommendations
Personal characteristics, low educational attainment, poor parental supervision and por support from teachers were identified as risk factors for teenage pregnancy. Most of the factors identified were modifiable. It is recommended that parents of adolescents be educated on the need for focusing on longer years of education for the adolescents and the need to improve communication between themselves and adolescents. The study has highlighted the need for a parenting education programme into the preventive care service package in the country. School curricular inputs on reproductive health for adolescent boys and girls should emphasize the disadvantages of teenage pregnancies. The supportive role of the teachers in solving problems of adolescents should be strengthened. The unmet need in contraceptive services for the married or cohabiting teenagers need to be addressed.
The risk factors identified by the study should be communicated to the PHM, so that they could focus their care on adolescents within families with the identified risk situations to prevent teenage marriages and pregnancies.
2940
References
- Chen X, Wen SW, Fleming N, Demissie K, Rhoads GG, Walker M. Teenage pregnancy and adverse birth a large population based retrospective cohort study. Int J Epidemiol 2007;36 (2):368-373.
- Smith GCS, Pell JP. Teenage pregnancy and risk of adverse perinatal outcomes associated with first and second births: population based retrospective cohort study. Br Med J 2001;323:476?79.
- United Nations Population Fund. MDG Linkages to UNFPA?s Work on Population, Reproductive Health and Women?s Empowerment . 2010.; Available from: https://www.unfpa.org/public/home/sitemap/icpd/MDGs/pid/6626 , Accessed 01/12/12.
- UNICEF. Fact Sheet: World Population Day. UNICEF Malaysia Communications; 2008; Available from: https://www.unicef.org/malaysia/Teenage_Pregnancies_-_Overview.pdf, Accesses 02/12/12.
- Kost K, Henshaw S. U.S. Teenage Pregnancies, Births and Abortions, 2008: National Trends by Age, Race and Ethnicity; Available from: www.guttmacher.org/pubs/USTPtrends08.pdf, Accessed 02/12/12.
- Avery L, Lazdane G. What do we know about sexual and reproductive health of adolescents in Europe? European Journal of Contraception and Reproductive Health Care 2008;13(1):58?70.
- United Nations Statistics Division. The World?s Women Reports, 2005; Available from: https://unstats.un.org/unsd/demographic/products/indwm/ww2005/tab2b.htm, Accessed 02/12/12.
- Acharya DR, Bhattarai R, Poobalan A, van Teijlingen ER, Chapman G. Factors associated with teenage pregnancy in South Aisa: a systematic review. Health Science journal 2010;4(1):3-14.
- Family Health Bureau. Reproductive Health Management Information System. Colombo, Sri Lanka: Family Health Bureau Ministry of Health, Sri Lanka; 2010.
- Department of Census and Statistics and Ministry of Healthcare & Nutrition. Sri Lanka Demographic and Health Survey 2006-2007. Department of Census and Statistics and Ministry of Healthcare & Nutrition; 2009.
- Millers BC, Benson B, Galbraith KA. Family Relationships and Adolescent Pregnancy Risk: A Research Synthesis. Developmental Review 2001;21(1):1-38.
- Imamura M, Tucker J, Hannaford P, da Silva MO, Astin M, Wyness L, Bloemenkamp KWM, Jahn A, Krro H, Olsen J, Temmerman M on behalf of the REPROSTAT 2 group. Factors associated with teenage pregnancy in the European Union countries: a systematic review. European Journal of Public Health 2007; 17(6): 630?36.
- Goonewardene IMR, DeeyagahaWaduge RPK. Adverse effects of teenage pregnancy.Ceylon Medical Journal 2005;50:116-120.
- Weerasekera D. Adolescent pregnancies-is the outcome different? Ceylon Medical Journal 1997;42: 16-17.
- Shrestha S. Socio-cultural factors influencing adolescent pregnancy in rural Nepal. International Journal of Adolescent Medicine & Health 2002;14:101-9.
- Hamilton BE, Ventura SJ. Birth Rates for U.S. Teenagers Reach Historic Lows for All Age and Ethnic Groups. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention National Center for Health Statistics, 2012: Available from: https://www.cdc.gov/nchs/data/databriefs/db89.pdf, Accessed 02/12/12.
- Abortion statistics for England and Wales, 2012: Available from: https://www.guardian.co.uk/news/datablog/2011/feb/22/teenage-pregnancy-rates-england-wales-map, Accessed 02/12/12.
- Sharma A, Verma K, Khatri S, Kannan A. Pregnancy in adolescents: a study of risks and outcome in Eastern Nepal. Indian Pediatrics 2001; 38: 1405-1409.
- Family Planning Association. Teenage pregnancy factsheet, 2010; Available from: https://www.fpa.org.uk/professionals/factsheets/teenagepregnancy, Accessed 02/12/12.
- Ventura SJ, Curtin SC, Abma JC. Henshaw SK. Estimated Pregnancy Rates and Rates of Pregnancy Outcomes for the United States, 1990?2008. National Vital; Statistics Reports, U.S. Department of Health and Human Services, Centers for Disease Control and Prevention National Center for Health Statistics, 2012: Available from: https://www.cdc.gov/nchs/data/nvsr/nvsr60/nvsr60_07.pdf, Accessed 02/12/12.
- Sharma A, Verma K, Khatri S, Kannan A. Determinants of pregnancy in adolescents in Nepal. Indian Journal of Paediatrics 2002; 69:19-22

