Keywords
Correspondence Analysis, Sanitation, Women’s Education, Social Development
Introduction
An important cause of death during the last two decades among children in developing countries continues to be diarrheal diseases.[1,2] According to Parashar et al.,[1] rotavirus causes approximately 111 million episodes of gastroenteritis requiring only home care, 25 million clinic visits, 2 million hospitalizations, and 352,000–592,000 deaths. Furthermore, by age 5, nearly every child will have an episode of rotavirus gastroenteritis resulting in death of approximately 1 in 293 rotavirus infections. The rotavirus which causes diarrhea in children is spread through fecal contamination of food and water supplies resulting from lack of adequate toilet facilities. According to the United Nations, lack of toilet facilities contributes to the deaths of some 700,000 children a year from diarrheal diseases.[3] These deaths are preventable. Furthermore, improving sanitary conditions is also desirable for social development given the fact that for every $1 spent on sanitation, productivity increases by $9 through better health outcomes. [3,4]
The failure of public programs and policies in most developing countries to address basic sanitation issues is indicated by the fact that between 1990 and 2008, the share of the world's population with access to basic sanitation increased only from 54 % to 61% and that even today nearly 2.6 billion people world wide have no toilet facilities.[5,6] The gravity of this issue led to the formulation of a Millennium Development Goal in 2000 to reduce the number of people without toilet facilities in developing countries by half. [3,7]
Lack of toilet facilities is a feminist issue.[8,9] Women in developing countries such as India resort to dehydration in order to cope with the woefully inadequate availability of public rest rooms for women. Women are also restricted in their capacity to maintain menstrual hygiene.[10,11] In spite of the fact that lack of toilet facilities poses a severe health hazard for children; result in depressing productivity levels nationally; and also disproportionately affect women’s capacity to maintain health and hygiene, empirical studies on toilet facilities remain few and far between.
Of the 2.6 billion people who lack toilet facilities, nearly 650 million live in India. Efforts toward addressing this gigantic problem of sanitation, appear to be bi-pronged involving both the government and the Non-Goverernmental Organization (NGO). The government programs have focused mainly on community campaigns. The main goal of this is to eliminate open defecation by 2017 through peer pressure, and to reward communities which achieve ‘open defecation free ‘ status. Of the many NGOs in the field of sanitation in India, Sulabh International is most well-known. Sulabh International has focused on providing a wide range of sanitation technologies at very affordable costs to the public. They have constructed thousands of 'pay & use public toilet-cum-bath’ complexes and more than a million pour-flush latrines in private houses. Though these strategies have proved to be effective in improving sanitary conditions, they do not focus on the individual level behavioral changes necessary to bring about desired levels of sanitation.[5,12]
In order to design public education programs to encourage healthy sanitary behaviors , it is necessary to assess the importance of education on sanitary practices in India. The purpose of this study is to examine the relationship between utilization of toilet facilities and educational levels , among women in India. We ask, ‘Do improvements in women’s education bring about changes in toilet facility utilization.’
Data
Data from the Third National Family Health Survey (NFHS-3) of India[13] is used in this study. NFHS is a large-scale, multi-round sample survey of households throughout India.[14] The NFHS has been conducted (a) to provide essential data on health and family welfare needed by the Ministry of Health and Family Welfare and other agencies for policy and program purposes, and (b) to provide information on important emerging health and family welfare issues.[14] The NFHS collected data on fertility, infant and child mortality, the practice of family planning, maternal and child health, reproductive health, nutrition, anemia, utilization and quality of health and family planning services of India. Since 1992-93, three rounds of the survey have been conducted including the latest survey, the NFHS-3 in 2005-06 which will be used in this study.
The NFHS-3 is a survey of over nationally representative sample of 124,385 women of age 15-49, and 74,369 men of age 15-54 from 109,041 households living in all 29 states.[14] The sample of NFHS-3 covers 99 percent of India’s population. In addition to the nationally representative sample, NFHS-3 also collected socioeconomic and health information on slum and non-slum populations from eight major Indian cities namely: Chennai, Delhi, Hyderabad, Indore, Kolkata, Meerut, Mumbai, and Nagpur.
NFHS-3 gathered individual level data from women and men as well as household data. The household questionnaire was used to interview the household head or any adult household member holding information about income and expenditure. Women were asked questions on fertility, marriage, reproductive experience and behavior, food and nutrition, health and hygiene practice, education, and gender relations. The interview of household and individuals also collected data on nutrition status such as, level of iodine in cooking salt, level of hemoglobin content in the blood of interviewed women, children and men, and measurement of Body Mass Index (BMI).[14] This study uses individual level data from women and focuses on two variables, educational level and type of toilet facilities. All cases with missing data on either of the two variables were dropped from the study. From a total sample of 124,385 available from NFHS-3, about 5662 cases with missing information, nearly 4.5 percent of the available data, were dropped to yield a sample of 118,733.
Data Analysis
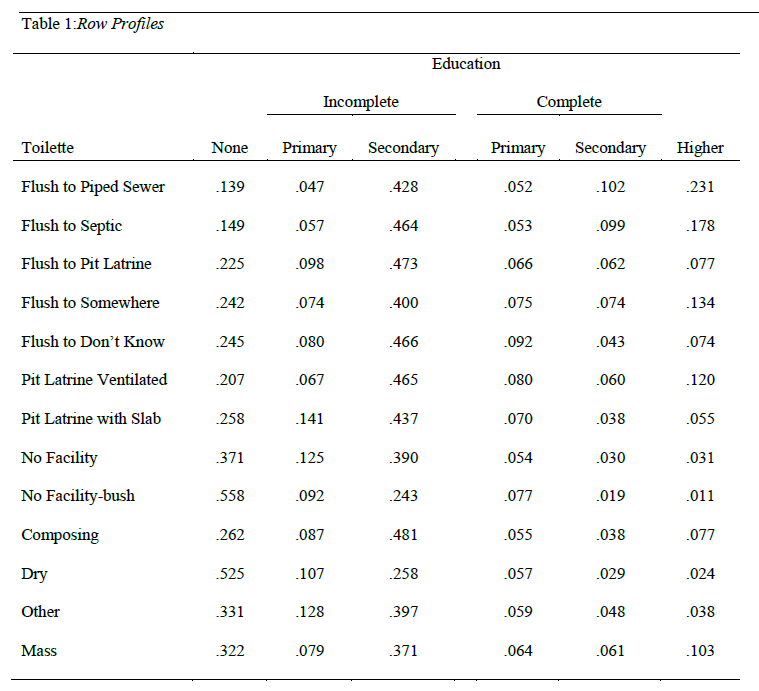
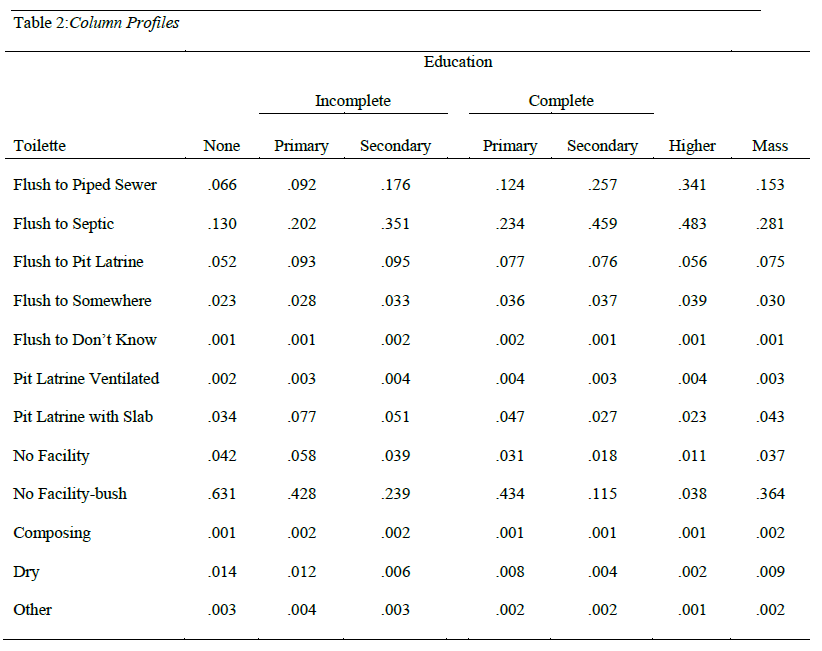
Correspondence analysis begins with calculation of two tables called ‘row profile’ and ‘column profile’ respectively. The row profiles are frequencies of row entries relative to their row total frequencies resulting in normalized rows. The column profiles are frequencies of column entries relative to their column total frequencies yielding normalized columns. These tables enable us to get first hand knowledge of the distribution of type of toilet facilities across various educational groups. Table 1 (column profile) shows that large proportions of respondents in the ‘no education ‘, almost 63 percent, have no toilet facilities. Nearly 34 percent of all who possess ‘flush to piped sewer’ facilities belong to the group of respondents with high levels of education (Table 2).
The goal of correspondence analysis is to reduce the complex details of the information available in the column and row profiles to measures of associations among various categories of the two variables, education, and type of toilet use. This approach is very similar to factor analytic methods where attempts are made to reduce the information in several variables to a few clusters (factors) of a small number of variables. In correspondence analysis, this is achieved by examining the data in the context of few ‘dimensions’ , usually two.
In many data reduction techniques such as principal component analysis, a minimum number of components is extracted to account for as much variance in the variables as possible. A similar approach is utilized in correspondence analysis as well. In correspondence analysis, a minimum number of dimensions is extracted to account for the maximum distances as possible among column and row categories. The distances are measured as ‘chi-squared distances’ which are weighted distances between normalized rows. Though there are several types of normalization methods, the symmetric normalization used in this analysis is particularly useful when the analytical focus is on examining the inter-relation among categories of the two variables, women’s educational level and type of toilet facility. The weights applied are inversely proportional to the square roots of the column totals.[15]
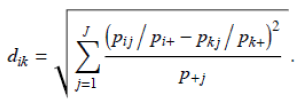
 = distance between two normalized rows, i and k.
= distance between two normalized rows, i and k.
 , where
, where  is the frequency at ith row and jth column and ‘n’ is the total number of respondents.
is the frequency at ith row and jth column and ‘n’ is the total number of respondents.
 , where
, where  is the frequency at ith row and kth column and ‘n’ is the total number of respondents
is the frequency at ith row and kth column and ‘n’ is the total number of respondents
J = total number of columns in the correspondence matrix
The chi-squared distances are examined to assess extent of dependencies among rows and columns in terms of the desired number of dimensions (usually 2). To continue the comparison made with principal component analysis (PCA), these dimensions are similar to the components in PCA. The amount of variance explained by each component in PCA is indicated by Eigen values. In correspondence analysis , the amount of variance in the chi-squared distances explained by dimensions is referred to as ‘inertia.’ Theoretically, the total chi-squared distance may be apportioned into as many columns and rows in the correspondence matrix. However in the interest of parsimony, the total chi –squared distance is assessed in terms of the number of dimensions , usually 2, as mentioned earlier. The maximum number of dimensions that can be extracted is a minimum of either (i -1)or( j -1) . The inertia associated with each row is the product of the row total (marginal frequencies or mass) and the square of its distance to the centroid (Yelland, 2010),  where
where 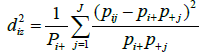 Rows and columns with large marginal frequencies influence the total of all inertias.[16]
Rows and columns with large marginal frequencies influence the total of all inertias.[16]
Results
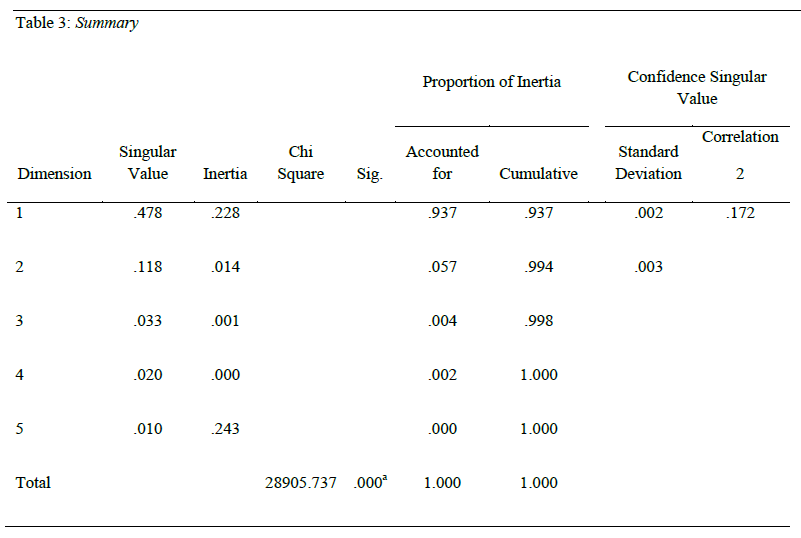
Table 3 presents the chi-square statistic along with the significance level. The chi-square statistic is 28905.737 significant at the .01 level. Of the five inertia values associated with the maximum number of dimensions possible (given by j-1), two have inertia values close to 0. The total of the five inertias amount to 24.3 percent with the first dimension contributing 22.8 percent. The second extracted dimension accounts for only 1.4 percent. The singular values presented in Table 3 are square root transforms of the inertias. The first and second dimensions account for about 93.7 percent and 5.7 percent respectively of the total variance (24.3 percent) explained by our model. These results suggest that a two dimensional model is adequate for explaining the relationship between categories of toilet types in use and women’s levels of education. Furthermore, knowledge of the distribution of the population across categories of education possibly accounts for 24.3 percent of the variance in the distribution of toilet facilities.
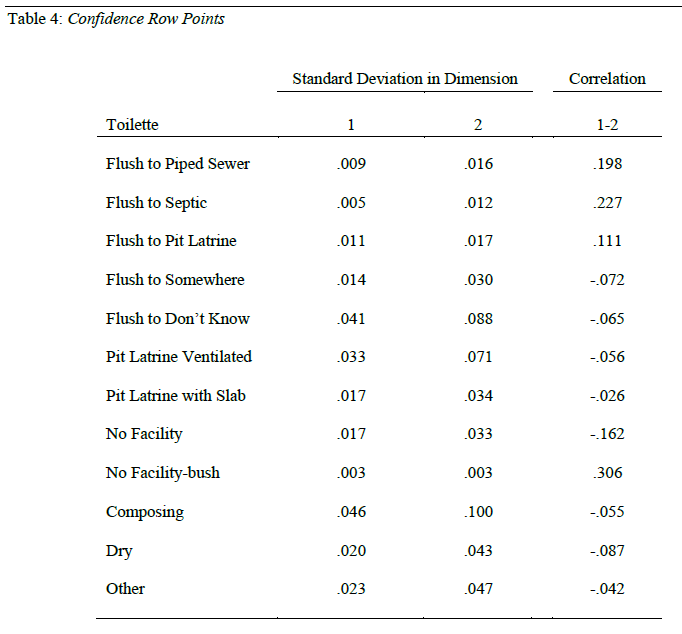
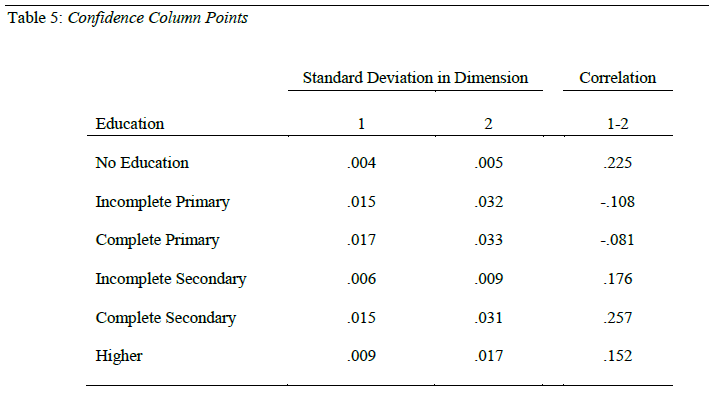
The confidences intervals for the estimates of row and column loadings on the extracted dimensions in correspondence analysis is known as ‘confidence statistics.’ Tables 4 and 5 present the confidence statistics for row, and column points respectively. The standard deviations for almost all the column and row points are small. In addition, the correlations between the dimensions for the scores range from low to moderate. These results suggest that correspondence analysis solutions obtained here are stable overall.
Perhaps the most important component of correspondence analysis procedures involves the plotting of dimension 1 against dimension 2 obtained under symmetric normalization of rows and columns. Figure 1 presents the biplot of the two dimensions. The biplot reveals several interesting patterns. The education category ‘no education’ is adjacent to ‘no toilet facility or bush’ and ‘dry toilet’. The neighborhood of ‘incomplete primary’ education is populated by several types of poor toilet facilities. The categories (types) of toilet facilities associated with ‘incomplete primary’ are ‘pit latrine with slab’ and ‘no facility’, ‘flush to pit latrine’, ‘composing toilet’, ‘others’ and ‘flush to don’t know’.
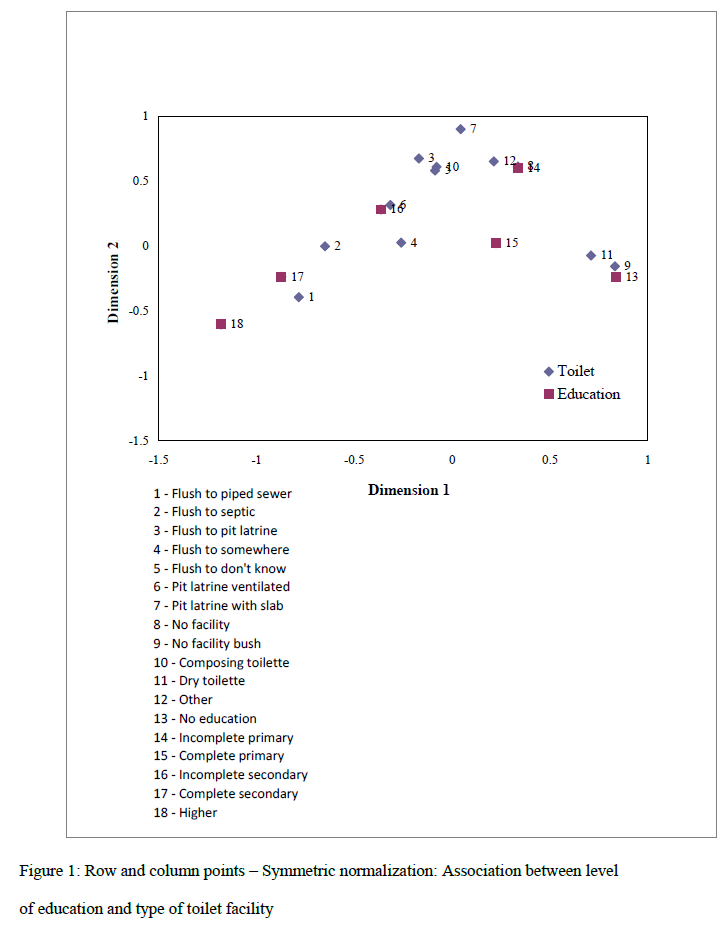
Figure 1: Row and column points – Symmetric normalization: Association between level of education and type of toilet facility
The category ‘complete primary’ is closely associated with ‘flush to somewhere’. Toilet facility types associated with ‘incomplete secondary’ is ‘pit latrine ventilated’. The category ‘complete secondary’ is associated with ‘flush to septic’. Finally, ‘high level of education’ is associated with ‘flush to piped sewer’.
Conclusion
In general, it appears that there is a positive association between level of education and quality of toilet facilities. With increases in women’s education, quality of toilet facility improves steadily. It is likely that general education brings about awareness and positive attitudes toward select use of sanitary toilet types. Enriching the curriculum at the secondary school level with facts and concepts of sanitation is likely to improve sanitary toilet practices. By explicitly discussing toilet practices, much of the shyness and reluctance to discuss and learn about toilet types that secure sanitary conditions necessary for healthy living may be reduced.
Behavioral changes are hard to accomplish unless either the felt needs or the interests of the target population with respect to sanitation are addressed. In generating interest, it is necessary to approach the topic by infusing emotional content and promoting ‘hope’ for better quality of life through sanitary toilet practices. Perhaps the most important component of health education is community participation. It is necessary to have a number of exhibition projects of sanitary toilet facilities set up in various communities .
The results of the present study should be considered in the context of its limitations. First, the study was limited to examining the association between two variables, women’s educational level and the type of toilet facility in use. Future studies may attempt to include controls in the proposed model in this study to asses the net effect of women’s educational levels on toilet type in use. Secondly, cultural and regional variations in sanitary practices in India were not considered. It is likely that many sub cultures within India promote sanitary practices for night soil disposal. It is necessary to learn about existing practices and knowledge among members of the target populations with respect to toilet practices. Such knowledge and traditions should be incorporated within health education campaigns to promote safe and sanitary toilet practices.
2767
References
- Parashar UD, Hummelman EG, Bresee JS, Miller MA, Glass RI. Global illness and deaths caused by rotavirus disease in children. Emerging Infectious Diseases 2003;(5):565-572.
- Ahs JW, Tao W, Löfgren L, Forsberg BC. Diarrheal diseases in low- and middle-income countries: Incidence, prevention and management. The Open Infectious Diseases Journal 2010; 4(4):113-124.
- Canaday C. Simple urine-diverting dry toilets built with recycled or readily available materials. Sustainable Sanitation Practice 2011;1(6):4-9.
- Okechukwu OI, Okechukwu AA, Noye-Nortey H, Owusu-Agyei. Toilet practices among the inhabitants of Kintampo District of Northern Ghana. Journal of Medicine and Medical Sciences 2012;3(8): 522-530
- Majra JP, Gur A .India needs a great sanitary awakening. Indian J Occup Environ Med. 2008;12(3):143-150.
- Moe CL, Rheingans RD. Global challenges in water, sanitation and health. Journal of Water and Health 2006;4(Suppl.):41-57.
- Bartram J, Cairncross S. Hygiene, sanitation, and water: Forgotten foundations of health. PLoS Medicine 2010;7(11): e1000367, doi:10.1371/journal.pmed. 1000367.
- Banks TL. Toilets as a feminist issue: A true story. Berkeley women's law journal 1990-1991;6(2):263-289.
- Wickramasinghe D. Managing menstrual hygiene in emergency situations: How far from reality? Bangladesh Development Journal 2012;9(2):31-56.
- Adinma E, Adinma J. Perceptions and practices on menstruation amongst Nigerian secondary school girls. African Journal of Reproductive Health 2009;8 (3):74-83.
- Omidvar S, Begum K. Factors influencing hygienic practices during menses among girls from south India- A cross sectional study. International Journal of Collaborative Research on Internal Medicine & Public Health 2010;2(12):411-423.
- Taneja DK. Health policies and programmes in India (4th ed.). Doctors Publications, New Delhi, 2004.
- International Institute for Population Sciences. Third National Family Health Survey (NFHS-3) of India. Mumbai, IIPS.2005-2006: Retrieved September 29, 2012 from https://www.rchiips.org/NFHS/data1.shtml.
- International Institute for Population Sciences (IIPS) and Macro International. National Family Health Survey (NFHS-3) India 2005-06. vol.1., IIPS, Bombay, 2006.
- Yelland PM. An introduction to correspondence analysis. The Mathematica Journal. 2012;4(1):1-24.
- Benzécri JP. Correspondence analysis handbook. Dekker, New York, 1992.

