Keywords
Sexual dysfunction; Male; Epilepsy; Ethiopiahamartomatous polyps
Abbreviations: AED: Antiepileptic Drug; CSFQ-M-C: Changes in Sexual Function Questionnaires for Male Clinical; ED: Erectile Dysfunction; HADS: Hospital Anxiety and Depression Scale; HSDD: Hypo sexual Desire Disorder; SD: Sexual Dysfunction; SSQ: Social Support Questionnaire
Introduction
Abbreviations: AED: Antiepileptic Drug; CSFQ-M-C: Changes in Sexual Function Questionnaires for Male Clinical; ED: Erectile Dysfunction; HADS: Hospital Anxiety and Depression Scale; HSDD: Hypo sexual Desire Disorder; SD: Sexual Dysfunction; SSQ: Social Support Questionnaire
The prevalence of epilepsy in Ethiopia is 5-8 cases per 1000 population with both incidence and prevalence was higher in males [6]. A study conducted among 912 Kenyans, showed that sexual dysfunction has a great impact on affecting the quality of life in both men and women patients with epilepsy [7]. A sexual dysfunction can be a disturbance in the subjective sense of pleasure or desire usually associated with sex, or by the objective performance [8,9]. It is more prevalent in males than in females [10]. Generally, prevalence is about 10% across all ages. The prevalence is over 50% in men between 50 and 70 years of age [11].
In a population based study, 21.15% of male and 14% of the female has been diagnosed to have one or more sexual disorder. The prevalence of erectile dysfunction reported to be 15.77%, hypoactive sexual desire disorder reported 2.56%, premature ejaculation has been found to be 8.76% of the male, and associated with various demographic characteristics like age and educational status [11]. The prevalence of sexual dysfunction in men and women with epilepsy is, 30 to 66% and 14 to 50% respectively [12]. Hypo sexuality is the predominant syndrome, which is characterized by the loss of sexual desire, reduced sexual activity, and inhibited sexual arousal [12].
Studies showed that due to sexual problems, male patients have a lower marriage rate and have fewer children than expected [13]. Many studies showed that sexual dysfunction has a negative effect on marital function. A reported case study indicated that 75% of couples in marital therapy are not satisfied with their sexual life, and from the report in sexual therapy marital discord affects sexual function [14].
Erectile dysfunction is the persistent inability to attain and maintain an erection sufficient to permit satisfactory sexual performance. Although erectile dysfunction is a benign disorder, it affects physical and psychosocial health and has a significant impact on the quality of life of sufferers and their partners [15].
In more than 60% of men who complain about erectile dysfunction due to organic reasons, especially endothelial and metabolic dysfunction like hypertension, coronary heart disease, hypercholesterolemia and diabetes mellitus [16]. Other reasons for developing sexual dysfunction are age, lifestyle, alcohol- and nicotine-abuse, obesity and drug-induced side effects [17].
Abnormalities in sexual function are common comorbid condition in patients with epilepsy, the risk increased fivefold as compared to general population [18]. Disturbance in sexuality signifies a major limitation in the quality of life and may have harmful effects on nearly all areas of life, which is a very important indicator of the patients health status [19-25]. Despite this, there is no published study in Ethiopia among male patients with epilepsy, Therefore, this study aimed to determine prevalence and associated factors of sexual dysfunction among male patients with epilepsy.
Methods and Materials
Study design and setting
An institutional based cross-sectional study was conducted from May 15- June 15, 2019. In the east Ethiopia there are nine public hospitals. The study was conducted in the three selected public hospitals (Hiwotfana specialized hospital, Jegol and Dilchora hospital). Hiwotfana hospital is one of the teaching hospitals in the Eastern part of Ethiopia. It is located in Harar at 525 km from Addis Ababa. Hiwotfana hospital serves the eastern partial population as a referral hospital. Jegol hospital is allocated in the walled part of Harar city; Ras Mekonin established this hospital around 1904 EC. The Dire dawa Dilchora hospital is 47 km far away from Harari.
Study population
The study participants were selected from all male patients with epilepsy, who had follow up in the selected public hospitals. All married and sexually active male patients with epilepsy were included in the study, whereas the male patients who had been unconscious, and unable to respond verbally were excluded.
Instruments
Structured interviewer administered questionnaire was used to measure, a socio-demographic questionnaire to assess the patients’ background information. Substance-related factors used to assess substance use history of the patient; similarly, clinical factors were assessed by yes/no answers of respondents. Social support was measured by the Oslo-3 scale. It has the sum score scale ranging from 3–14 [21].
Sexual dysfunction was measured by using Changes in Sexual Functioning Questionnaires (CSFQ-M-C) Clinical Version. It contains 14 items and was used to assess the presence/absence of sexual dysfunction in the study participants. The questionnaire has scored five likert scales for answers, and all the 14 items were answered. Score of ≤ 47(14 to 70) indicate global sexual dysfunction. The questionnaires contain pleasure (item 1), desire /frequency (item 2 & 3), desire/interest (item 4, 5 & 6), erection (item 7, 8 & 9), orgasmic/ejaculation (item 11, 12&13). The current study had Cronbach’s α of 0.90 [23].
Psychological distress was measured by Kessler Psychological Distress Scale (K10), which score a total score of < 20 was considered normal; 20-24 mild distress; 25-29 moderate distress; and 30-50 severe distress with 5 possible responses for each question ranged from ‘none of the time’ (score 1) to ‘all of the time’ (score 5). In this study, the scores will be dichotomized into those who scored<20 (absence of psychological distress) and those who scored≥20 (presence of psychological distress) [22].
Current substance use: thoseparticipants used at least one of a specific substance for non-medical purpose within the last three months (alcohol, khat, tobacco, others). Data was collected using face to face interview methodes and chart review. Six male professional nurses for data collectors and supervised by three psychiatry nurses. The training was given for data collectors and supervisors.
Sample size determination and study procedures
Sample size was determined by using Single population proportion formula.


Adding 10% non-response rate gives us a final sample size of 581
Where,
n= Minimum sample size required for the study
Z= Standard normal distribution (Z=1.96) with confidence interval of 95% and α=0.05
P= Proportion of sexual dysfunction 67.4% was taken from a study which is done in Addis Ababa, Ethiopia in Amanuel mental specialized hospital [24].
d= Absolute precision or tolerable margin of error (d) =4%=0.04
Concerning the sampling technique which was employed in the study was systematic random sampling. The study population comes from selected three public hospitals; these include, Hiwotfana, Jegol and Dilchora. Study population was selected proportionally, from each hospital (Figure 1).
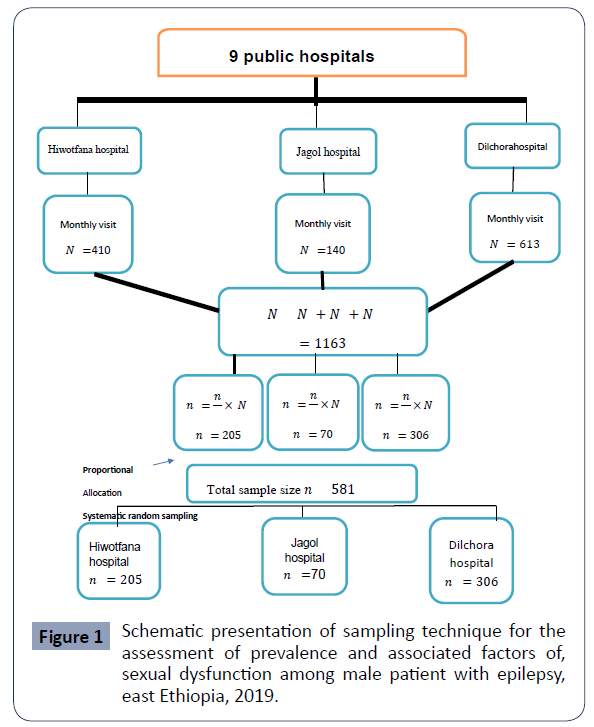
Figure 1 Schematic presentation of sampling technique for the assessment of prevalence and associated factors of, sexual dysfunction among male patient with epilepsy, east Ethiopia, 2019.
Systematic random sampling was used to select study subjects from each hospital. The interval size (k) was calculated using the following formula.


Therefore, the interval size for each hospital was two. So that every two person was selected from the study population.
Where
N-Monthly population of selected hospitals
n- Sample size of each hospital (proportionally allocated)
Statistical analysis
Data was cleaned, coded and entered using Epidata version 3.1 and analyzed using SPSS-20 respectively. The descriptive data were summarized using tables. Associations of sexual dysfunction and factors were identified using logistic regression analyses. Following each bi-variable regression, multivariable logistic regression model was constructed. P-value less than 0.05 were considered as statistically significant and the strength of association was determined using adjusted odds ratio (AOR) at 95% CI.
Results
Socio-demographic characteristics of the respondents
Of the total 581 study participants, 572 were interviewed yielding a response rate of 98.5%. Respondents’ age ranged from 18 to 60 years with a median age of 31 years, with an inter quartile range of 12 years. 44.2% were in the age group of 25–34 years. About 42.7% of the respondents were single, 67% were Muslim followers, concerning occupation, 27.4% were farmers and 10.7% were not employed at the time of the study. Regarding educational status, 39.2% attended secondary school followed by primary school 34.4% (Table 1).
| Variable |
Frequency |
Percentage |
| Age |
| 18 - 24 |
108 |
18.9 |
| 25 - 34 |
253 |
44.3 |
| 35 - 44 |
134 |
23.4 |
| >=45 |
77 |
13.5 |
| Religion |
| Muslim |
383 |
67.0 |
| Orthodox |
117 |
20.5 |
| Protestant |
72 |
12.6 |
| Marital status |
| widower |
44 |
7.7 |
| Married |
463 |
80.9 |
| Divorced |
65 |
11.4 |
| Ethnicity |
| Oromo |
226 |
39.5 |
| Amhara |
138 |
24.1 |
| Harari |
100 |
17.5 |
| Somali |
60 |
10.5 |
| Others* |
48 |
8.4 |
| Educational status |
| Not read & write |
91 |
15.9 |
| Primary |
197 |
34.4 |
| Secondary |
224 |
39.2 |
| College above |
60 |
10.5 |
| Occupation |
| Farmer |
157 |
27.4 |
| Merchant |
143 |
25.0 |
| Employee |
98 |
17.1 |
| Unemployed |
61 |
10.7 |
| Student |
67 |
11.9 |
| Daily laborer |
46 |
8.0 |
Others*=Debube, Gurage
Table 1 Socio demographic characteristics of male patients with eplepsy at bublic hospitals, east Ethiopia, 2019 (n=572).
Clinical characteristics of respondents
From a total of 572 respondents, 38.3% have been living with epilepsy for 6-10 years followed by 31.3% have been lived ≥11 years. Concerning the age of onset of epilepsy, 50.3% were found between age group of 20 – 29 years. The majority of the respondents, 57.9% had one or more seizure attacks per month, around 53.3% of patients with epilepsy were on polytherapy (two or more antiepileptic drugs). The most prescribed AED was 16.4% phenobarbitone (16.4%) followed by phenytoin (12.8%). Among the respondents, 4.9% and 6.5% had past mental illness and chronic medical illness respectively. Around 13.1% of epileptic patients had frequent relational problems with their partners (Table 2).
| Variables |
Frequency |
Percent (%) |
| Duration of illness |
| ≤5 years |
174 |
30.4 |
| 6-10 years |
219 |
38.3 |
| ≥11 years |
179 |
31.3 |
| Age at onset of illness |
| 10-19 years |
87 |
32.7 |
| 20-29 years |
288 |
50.3 |
| ≥30 years |
97 |
17 |
| Frequency of seizure |
| ≥1/month |
331 |
57.9 |
| 1-3/year |
166 |
29 |
| Seizure free for year |
75 |
13.1 |
| Type of drugs |
| One |
267 |
46.7 |
| ≥two |
305 |
53.3 |
| Medication duration |
| ≤5 years |
306 |
53.5 |
| 6-10 years |
167 |
29.2 |
| ≥11 years |
99 |
17.3 |
| Family history of mental illness |
| Yes |
44 |
7.7 |
| No |
528 |
92.3 |
| Chronic medical illness |
| Yes |
37 |
6.5 |
| No |
535 |
93.5 |
| Past mental illness |
| Yes |
28 |
4.9 |
| No |
544 |
95.1 |
| Types of seizure |
| GTC |
364 |
63.6 |
| Partial/ complex partial |
194 |
33.9 |
| Absence |
14 |
2.4 |
| Controlled seizure |
| Yes |
222 |
38.8 |
| No |
350 |
61.2 |
| Relational problem |
| Yes |
75 |
13.1 |
| No |
497 |
86.9 |
| Psychological distress |
| yes |
318 |
55.6 |
| No |
254 |
44.4 |
Table 2 Description of clinical factors among male patients with epilepsy visiting outpatient clinics at public hospitals, east Ethiopia, 2019(n=572).
Lifetime and current substance use among respondents
Around 75.9% of respondents had a history of current substance use. Among the participants 55.1% and 15.6%) were using khat and tobacco respectively (Table 3).
| Variables |
Frequency |
Percent |
| Ever used khat |
| Yes |
376 |
65.7 |
| No |
196 |
34.3 |
| Ever used alcohol |
| Yes |
136 |
23.8 |
| No |
436 |
76.2 |
| Ever used tobacco |
| Yes |
201 |
35.1 |
| No |
371 |
64.9 |
| Current khat user |
| Yes |
315 |
55.1 |
| No |
257 |
44.9 |
| Current alcohol user |
| Yes |
30 |
5.2 |
| No |
542 |
94.8 |
| Current tobacco user |
| Yes |
89 |
15.6 |
| No |
483 |
84.4 |
Table 3 Substance use characteristics of participants among male patients with epilepsy visiting outpatient clinics at public hospitals, east Ethiopia, 2019(n=572).
Prevalence of sexual dysfunction among patients with epilepsy
The prevalence of global sexual dysfunction was found to be 59.4 % with 95% CI of (57.6, 64.9)of the respondents.
Factors associated with sexual dysfunction among male patients with epilepsy
In multivariable analysis age, current chat use, uncontrolled seizure, and psychological distress were found to be significantly associated with sexual dysfunction at a p-value less than 0.05.
Concerning age, those ≥ 45 years were 5 times more likely to have sexual dysfunction compared to whose age less than 45 years AOR=5.43, 95% CI (1.22,7.18). The odds of having sexual dysfunction among participant with current khat users were about 3.59 times higher than responders who did not use khat(AOR=3.59, 95% CI 2.17, 5.93). Epileptic patient whose seizure was uncontrolled has 3 times more likely to develop sexual dysfunction as compared to controlled seizure (AOR=3.10, 95% CI 1.83, 5.29). The odds of having sexual dysfunction among respondents with psychological distress were 2 times higher as compared to respondents who did not have psychological distress (AOR=2.01, 95% CI 1.19, 3.38) (Table 4).
| Explanatory variables |
Sexual dysfunction |
COR, (95% CI) |
AOR, (95% CI) |
| Yes(N) |
No |
| Age 18 – 24 |
58 |
50 |
1 |
1 |
| 25 – 34 |
171 |
82 |
1.79 (1.13, 2.85) |
2.43(0.01,5.83) |
| 35 - 44 |
101 |
33 |
2.63 (1.53, 4.55) |
2.72(0.89, 8.23) |
| ≥ 45 |
67 |
10 |
5.77(2.69, 12.41) |
5.43(1.22, 7.18)** |
| Educational status |
| Unable to read & write |
73 |
18 |
3.79(1.84, 7.82) |
3.50(0.16, 10.55) |
| Primary |
156 |
41 |
3.56(1.93, 6.57) |
2.58(1.05, 6.35) |
| 9-12 |
137 |
87 |
1.47(0.83, 2.61) |
1.60(0.68, 3.76) |
| College and above |
31 |
29 |
1 |
1 |
| Occupation |
| Farmer |
120 |
37 |
2.05(1.18, 3.55) |
1.40(0.61, 3.17) |
| Merchant |
98 |
43 |
1.47(0.85, 2.53) |
1.08(0.51, 2.29) |
| Daily laborer |
34 |
12 |
1.79(0.82, 3.88) |
1.05(0.38,2.90) |
| Student |
34 |
33 |
0.65(0.34, 1.22) |
0.61(0.24, 1.53) |
| Unemployed |
49 |
12 |
2.58(1.22,5.47) |
1.82(0.70, 4.71) |
| Government employee |
60 |
38 |
1 |
1 |
| Social support |
| Poor social support |
186 |
65 |
3.36(1.66, 6.81) |
5.51(0.95, 15.62) |
| Moderate social support |
193 |
90 |
2.53(1.26,5.07) |
2.27(0.81,6.31) |
| Strong social support |
18 |
20 |
1 |
1 |
| Current khat user |
| Yes |
257 |
58 |
3.70(2.54,5.39) |
3.59(2.17,5.93) ** |
| No |
140 |
117 |
1 |
1 |
| Psychological distress |
| Yes |
245 |
73 |
2.25(1.57, 3.24) |
2.01(1.19,3.38)*** |
| No |
152 |
102 |
1 |
1 |
| Chronic medical illness |
| Yes |
31 |
6 |
2.38(0.97,5.82) |
0.53(0.14,1.93) |
| No |
366 |
169 |
1 |
1 |
| Age of onset of epilepsy |
| 10 – 19 |
116 |
71 |
3.36(1.66, 6.81) |
1.37(0.76, 2.49) |
| 20 - 29 |
207 |
81 |
2.53(1.26, 5.07) |
0.91(0.32,2.58) |
| ≥30 |
74 |
23 |
1 |
1 |
| Duration of epilepsy |
| ≤5 year |
100 |
74 |
1 |
1 |
| 6-10 year |
149 |
70 |
1.57(1.04, 2.38) |
1.17(0.55, 2.51) |
| ≥ 11 year |
148 |
31 |
3.53(2.16, 5.76) |
1.35(0.43, 4.19) |
| Seizure frequency |
| ≥1/month |
258 |
73 |
4.49(2.66, 7.60) |
1.50(0.68, 3.32) |
| 1 – 3 /year |
106 |
60 |
2.25(1.29, 3.92) |
1.23(0.53,2.85) |
| Seizure free/year |
33 |
42 |
1 |
1 |
| Seizure controlled |
| Yes |
129 |
93 |
1 |
1 |
| No |
268 |
82 |
2.35(1.63, 3.39) |
3.11(1.83, 5.29)** |
| Seizure type |
| Tonic-clonic seizure |
249 |
114 |
3.94(1.29, 12.04) |
3.08( 0.59,16.12) |
| Partial/complex partial |
142 |
52 |
4.91(1.57, 15.34) |
2.34(0.44, 41) |
| Absence |
6 |
9 |
1 |
1 |
| Medication |
| Monotherapy |
158 |
109 |
1 |
1 |
| Polytherapy |
239 |
66 |
2.49(1.73, 3.60) |
4.32(0.64, 11.38) |
| Treatment duration |
≤5 year
6 – 10 y |
189
122 |
117
45 |
1
1.67(1.11, 2.53) |
1
1.25(0.60, 2.61) |
| ≥ 11 year |
86 |
13 |
4.09(2.18, 7.66) |
0.91(0.27, 3.02) |
| Antiepileptic drug |
| phenobaribtone |
44 |
50 |
1 |
1 |
| Phenytoine |
39 |
34 |
1.30(0.70, 2.40) |
0.68(0.28, 1.62) |
| Carbamazepine |
38 |
12 |
4.02(1.84, 8.80) |
3.04(0.15, 7.99) |
| Sodium valproate |
37 |
13 |
2.92(1.39, 6.11) |
3.00(0.14, 7.88) |
Chi square= 5; degree of freedom=8; Hosmer Lemeshow test= 0.726; AED=Anti Epleptic Drug *p-value less than 0.05 **p-value less than 0.001
Table 4 Bivariable and multivariable binary logistic regression analysis showing association between factors and sexual dysfunction among male patients with epilepsy visiting outpatient clinics public hospitals, east Ethiopia, 2019(N=572).
Discussion
In this study the prevalence of global sexual dysfunction was 59.4 % with 95% CI of (57.6, 64.9),which is in line with the study conducted in Norway reported 63.3% [26].
However, the result of this study is higher than the study conducted in Bangalore and Iran which was 38% and 42.5% respectively [27-29,30-34]. The possible reason for this significant difference may be explained by the difference in measurement instrument, which also excludes the patients with hypertension, DM, hyper or hypothyroidism, urologic disease and other known neurologic disorder and mental illnesses, whereas our study includes all except unconscious and unable to communicate [35-39].
In this study; age greater than 45 years were five times more likely to develop sexual dysfunction as compared to younger ones’, which is supported by the study done in Addis Ababa [24] and Kenya [34,38]. This might be also due to hormonal changes resulted from decreased body function due to advanced age and enzyme inducing AED which might cause testosterone level depletion [28,30].
The study indicated that uncontrolled seizure was three times more likely to develop sexual dysfunction as compared to controlled seizure. This might be people with epilepsy had a much smaller increase in genital blood flow, a key factor in sexual arousal [39]. Men with epilepsy are known to have greater risk for erectile dysfunction and the side effect of AED also a risk for sexual dysfunction [34,35]. This finding is supported by the study conducted in Egypt [33].
In this study, having psychological distress was two times more likely to develop sexual dysfunction as compared to counterpart. This finding is supported by study conducted in the Japan [37]. The possible reason might be blood flow to the sex organ can be disturbed in persons with psychological distress due to neurochemical imbalance [36]. Regarding substance use; current khat user was 3.59 times more likely to develop sexual dysfunction as compared to non-users. This finding was supported by the study conducted in Amanuel mental specialized hospital [24]. The possible reason might be chewing khat is considered a cause of psychosis because khat contains some stimulating elements that may affect erectile dysfunction [31,32].
The strength of this study is; standardized tools were used to assess outcome variable and independent variables like psychological distress. Some of the limitations are social desirability bias due to sensitivity of the questionnaires; in addition, this study didn’t identify specific type of sexual dysfunction and didn’t compare control and case. This study only determines the prevalence and associated factors of global sexual dysfunction in male patients with epilepsy.
Conclusion
The predictors for sexual dysfunction of male patients with epilepsy are; age, uncontrolled seizure, current khat use and psychological distress. The question of sexual activity should be raised by health-care professionals as a routine part of the management of patients with epilepsy and needs to refer to psychiatry clinic.
Declarations
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Institutional Review Board of the College of Health Sciences of University of Gondar and Amanuel Mental Specialized Hospital. A formal letter of permission was obtained from zonal administrative office. Informed consent and assent was secured from each participant during the study period. Participants gave the written informed consent. After having adequate information about the study, the potential benefits had been provided. Participants who were found sexual dysfunction positive during the study, communication to the nearby psychiatric clinic was done in order to have further assessment of their condition
Consent for Publication
Not applicable
Availability of Data and Materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Competing Interests
The authors declare that they have no competing interests.
Funding
Not applicable
Authors’ Contributions
BS conceived the research idea, framed the methods, did the analysis, and wrote the final paper. SY, TF and AK participated in framing the method, data collection, and write-up. DM wrote the manuscript, framing the method and write-up. All the authors read and approved the final manuscript.
Acknowledgments
Authors of this study would like to acknowledge the entire staff of the public hospitals and managers for their cooperation. Our sincere gratitude goes to University of Gondar, College of Medicine and Health Sciences, department of Psychiatry and Amanuel Mental Specialized Hospital, Research and Dissemination Office for funding the study. We also appreciate the study participants for their cooperation in providing the necessary information.
37780
References
- Heyne HO, Singh T, Stamberger H, Jamra RA, Caglayan H, et al. (2018) De novo variants in neurodevelopmental disorders with epilepsy. Nat Genet 50:1048-1053.
- Ngugi AK BC, Kleinschmidt I, Sander JW, Newton CR (2010) Estimation of the burden of active and life‐time epilepsy: a meta‐analytic approach. Epilepsia 51:883-890.
- Ngugi AK, Bottomley C, Kleinschmidt I, Wagner RG, Kakooza-Mwesige A, et al. (2013) Prevalence of active convulsive epilepsy in sub-Saharan Africa and associated risk factors: cross-sectional and case-control studies. Lancet Neurol12:253-263.
- Sander JW, Shorvon SD (1996)Epidemiology of the epilepsies. J Neurol Neurosurg Psychiatry 61:433-433.
- Paul A, Adeloye D, George-Carey R, Kolčić I, Grant L, et al. (2012) An estimate of the prevalence of epilepsy in Sub–Saharan Africa: A systematic analysis. J Glob Health 2: 020405.
- Tekle-Haimanot R, Abebe M, Gebre-Mariam A, Forsgren L, Heijbel J, et al. (1990) Community-based study of neurological disorders in rural central Ethiopia. Neuroepidemiology 9:263-277.
- Edwards T, Scott AG, Munyoki G, Odera VM, Chengo E, et al. (2008) Active convulsive epilepsy in a rural district of Kenya: a study of prevalence and possible risk factors. Lancet Neurol 7:50-56.
- Taubøll E, Luef G (2008) Gender issues in epilepsy—the science of why it is special. Seizure 17:99-100.
- Hamed SA, Hermann BP, Moussa EMM, Youssef AH, Rageh TA, et al. (2015) Evaluation of penile vascular status in men with epilepsy with erectile dysfunction. Seizure 25:40-48.
- Sadock BJ,Sadock VA, Ruiz P (2011) Kaplan and Sadock's synopsis of psychiatry. Behavioral sciences/clinical psychiatry: Lippincott Williams & Wilkins.
- Althof SE, O'Leary MP, Cappelleri JC, Crowley AR, Tseng LJ, et al. (2006) Impact of erectile dysfunction on confidence, self-esteem and relationship satisfaction after 9 months of sildenafil citrate treatment. J Urol176: 2132-2137.
- Rao TSS, Darshan MS, Tandon A (2015) An epidemiological study of sexual disorders in south Indian rural population. Indian J Psychiatry 57:150-157.
- Atif M, Sarwar MR, Scahill S (2016) The relationship between epilepsy and sexual dysfunction: a review of the literature. Springerplus 5:2070.
- Webber MP,Hauser WA, Ottman R, Annegesr JF (1986) Fertility in persons with epilepsy: 1935–1974. Epilepsia 27:746-752.
- Hellmis E (2008) Sexual problems in males with epilepsy—An interdisciplinary challenge. Seizure 17:136-140.
- Trudel G, Goldfarb M (2010) Marital and sexual functioning and dysfunctioning, depression and anxiety. Sexologies 19:137-142.
- Hatzimouratidis K, Amar E, Eardley I, Giuliano F, Hatzichristou D, et al. (2010) erectile dysfunction and premature ejaculation. Eur Urol 57:804-814.
- Laumann EO, Paik A, Rosen RC (1999) Sexual dysfunction in the United States: prevalence and predictors. JAMA 281: 537-544.
- Feldman HA Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB (2002) Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol 2:278-280.
- Vallancien G, EmbertonM, Harving N, van Moorselaar RJA, Alf-One Study Group (2003) Sexual dysfunction in 1,274 European men suffering from lower urinary tract symptoms. J Urol 169:2257-2261.
- Abiola T, Udofia O, Zakari M (2013) Psychometric properties of the 3-item oslo social support scale among clinical students of Bayero University Kano, Nigeria. J Malaysian Journal of Psychiatry 22:32-41.
- Andrews G, Slade T (2001) Interpreting scores on the Kessler psychological distress scale (K10). Australian and Aust N Z J Public Health 25:494-497.
- Garcia-Portilla MP,SaizPA, Fonseca E, Al-Halabi S, Bobes-Bascaran MT, Arrojo M, et al. (2011) Psychometric properties of the Spanish version of the Changes in Sexual Functioning Questionnaire Short-Form (CSFQ-14) in patients with severe mental disorders. J Sex Med 8:1371-1382.
- Radić B, UL, Juren-Meaški S, Svilokos-Brataljenović N, Radić P, et al. (2013) Erectile dysfunction in patients with neurologic disorders. JNC 62:1-2.
- Henning OJ, NakkenKO, Træen B, Mowinckel P, Lossius M (2016) Sexual problems in people with refractory epilepsy. Epilepsy Behav 61:174-179.
- Bener A, Al-Ansari A, Afifi M, Krishna PV (2007) Erectile dysfunction among hypertensive men in a rapidly developing country. Indian J Urol 23: 109–113.
- Keller J, Chen YK, Lin HC (2012) Association between epilepsy and erectile dysfunction: Evidence from a population‐based study. J Sex Med 9:2248-2255.
- Nikoobakht M, Motamedi M, Orandi A, Meysamie A, Emamzadeh A (2007) Sexual dysfunction in epileptic men. Urol J 4:111-117.
- Zhao S,Tang Z, Xie Q, Wang J, Luo L, et al. (2019) Association between epilepsy and risk of sexual dysfunction: A meta-analysis. Seizure 65: 80-88.
- Hamed SA,Hermann BP, Moussa EMM, Youssef AH, Rageh TA, et al. (2015) Evaluation of penile vascular status in men with epilepsy with erectile dysfunction. Seizure 25:40-48.
- Schouten BWV, Bosch JLHR, Bernsen RMD, Blanker MH, Thomas S (2005) Incidence rates of erectile dysfunction in the Dutch general population. Effects of definition, clinical relevance and duration of follow-up in the Krimpen Study. Int J Impot Res 17:58-62.
- Hamed SA (2016) The effect of epilepsy and antiepileptic drugs on sexual, reproductive and gonadal health of adults with epilepsy. Expert Rev Clin Pharmacol 9:807-819.
- Seid A,GerenseaH, Tarko S, Zenebe Y, Mezemir R (2017) Prevalence and determinants of erectile dysfunction among diabetic patients attending in hospitals of central and northwestern zone of Tigray, northern Ethiopia: a cross-sectional study. BMC Endocr Disord 17: 16.
- Morrell MJ, SperlingMR, Stecker M, Dichter MA (1994) Sexual dysfunction in partial epilepsy: a deficit in physiologic sexual arousal. Neurology44:243.
- Goldfarb MR, TrudelG, Boyer R, Préville M (2007) Marital relationship and psychological distress: Its correlates and treatments. Sexual and RelationshipTherapy 22:109-126.
- Sugimori H, Yoshida K, Tanaka T, Baba K, Nishida T, et al. (200) Relationships between Erectile Dysfunction, Depression, and Anxiety in Japanese Subjects. The Journal of Sexual Medicine 2: 390-396.
- Geoffrey MU (2011) The Prevalence Of Sexual Dysfunction Among Patients With Diabetes Mellitus Attending The Outpatient Diabetic Clinic At Kenyatta National Hospital. University of Nairobi Research Archive.
- Mattson RH,Cramer JA, Collins JF (1992) A comparison of valproate with carbamazepine for the treatment of complex partial seizures and secondarily generalized tonic-clonic seizures in adults. The Department of Veterans Affairs Epilepsy Cooperative Study No. 264 Group. N Engl J Med 327: 765–771.

