Keywords
Rural women; Contraceptive use; Socio- Economic; Reproductive health; Development
Introduction
There's a more significant need to increase the number of women incorporated in the development discourse, projects and programs at all levels of organization. This should be possible to guarantee that development programs address issues which influence women, related to their multiple roles in production and reproduction. The United Nations SDGs (Goal 3) calls for improvement of maternal health by lessening maternal mortality by seventy five percent and accomplishing general access to reproductive health (Contraceptive prevalence rate) and this demonstrates the high requirement for enhancing women's health since they are for the most part influenced all the while. Coupled to the above, SDGs expect to accomplish widespread access to Sexual and Reproductive health care services by 2030 and this incorporates the requirement for family planning data and information, and the joining of reproductive health into national programs and projects.
Uganda is one of the exceptionally populated on the planet and this is for the most part because of the high fertility rates which have handled her in a condition of great neediness, putting the government in high consumptions than funds. High population growth rates accompany a great deal of unfriendly impacts that put the nation at danger of unemployment and underdevelopment combined with other related variables. The real reason for this study is to connect the endeavors and the reality on ground to address the developing number of individuals in the nation, yet particularly taking a look at it from the reproductive health point of view in matters concerning contraceptive or procurement of family arranging benefits particularly to the rural women.
Background of the Research
The expanding utilization of contraception has empowered couples to pick the number and dispersing of their children and has enormous life sparing advantages since women and men are given decisions on when, where and how to characterize their sexual life and labor. Be that as it may however, the striking additions in making these advances accessible to the general population, contraceptive use is still low and the requirement for contraception is high in a portion of the world's poorest and most populous places.
All around, contraceptives keep expected 2.7 million newborn child mortality and the loss of 60 million of healthy life in a year [1-3]. A few studies demonstrate that advancement of family arranging in nations with high birth rates can diminish destitution and hunger and forestall 32% of every single maternal demise and about 10% of adolescent deaths [4,5]. Preventative use in the United States is practically widespread among women of reproductive age; 98% of all women who had ever engaged in sexual relations had utilized the male condom, 82% had ever utilized the oral prophylactic pill, and 56% had a partner who utilized pull back (UN Department of Economics and Social Affairs, 2014). The 2000/2001 World Development Report showed that half of young females on the planet reported being sexually dynamic by age 18 years.
Besides, the utilization of modern contraceptives in most African nations remains low whereby fertility, unmet requirement for contraception and population growth are high. 30% of all women are assessed to utilize conception prevention, although over half of every single African woman might want to utilize contraception in the event that it was accessible [5,6]. Over the previous years, the calls for including women in reproductive health issues have stressed the part of women in enhancing the health of their families and themselves [7]. Sexual and reproductive health was emphatically influenced by sex standards, whereby standards favored male youngsters and advancing women's monetary reliance on men, consequently adding to high rates of ripeness in numerous settings. Chabikuli et al. [8] recognizes that women and young ladies overall who neglected to arrange sex, condom use or monogamy on equivalent terms left them at a high hazard for undesirable pregnancies, disease and passing from pregnancy related causes and STIs. Birth control measures lessen quick population growth rates and bring up a genuine population issue. Rapid population growth and over population have stayed topical issues of incredible worry to numerous national governments and the universal group [4]. There has been a tendency of connecting specifically or by implication high population growth rates, particularly in the face of low profitability, with various types of social issues extending from destitution, scarcity of land, hunger and ecological degradation to political unsteadiness.
In addition, women and men in Uganda are known to be poor users of contraceptives especially in the rural areas though it is evident that knowledge about them has increased steadily [6,7]. The low use could however be accredited to accessibility and affordability which sometimes the women cannot manage coupled with the lack of knowledge on contraceptive use. While the maternal mortality rate is estimated at 435 for every 100,000 women giving birth, Uganda’s total fertility rate (TFR) of about 6.7 children per woman remains one of the highest in the world [9], for that reason, Uganda has population growth rates of about 3.2% per annum, the third highest in the world.
In this case, a wide range of studies have linked the importance of female education in reducing fertility rates and the general improvement in labor force participation and social welfare [8]. Other factors that play a role are urban-rural residence, women’s work and status, women’s status relative to men, religion, culture and taboos, age (difference between young women and old women), education level of the husband, household standard of living (economic or wealth status), influence of the mass media and community development in form of social networks [3,6,8,10-13].
It is therefore from the above background that the study lays out the importance of CU in the wellbeing of women and the country at large. The development process from the global world should be known to the local population and make them own the development process. Programs directed towards development should be grass root oriented because most interventions are purposed for the hard to reach population and they know what affects them better.
Feminist perspective, gender and development approach (GAD)
The Gender and Development approach to women empowerment rose in the 1980s from the grassroots authoritative encounters and compositions of the third world women's activists. This methodology additionally acquires/borrows from the encounters and examination of western feminists’ socialists worries with development issues [14-16]. The methodology further requires a blend of issues of realist political economy and the radical-women's activist issues of patriarchy and philosophy (patriarchal belief system). Sketching from the socialist-feminist perspective on social stratification in the public arena, the GAD approach contends that women's status in the public eye is seriously influenced by their material states of life and by their place in the national, local and worldwide economies. Women are significantly influenced by the way of patriarchal force in their social orders at the national, group and family unit levels. Furthermore, women's material conditions and patriarchal power are exclusively characterized and kept up by the acknowledged standards and qualities that characterize women's and men's parts and obligations in a specific culture [17].
GAD recognizes effects of development strategies and practices on women and men and views women as active specialists, not just as beneficiaries of the development process. It in this way raises doubt about both sex relations and the development process. Within the GAD perspective, a distinction is drawn between women’s interests in biology as a homogeneous entity and gender interests as socially constructed. From the above, gender orientation interests can be either practical or strategic [15]. Reasonable practical gender needs emerge out of existing conditions; these are prompt essential needs, for example, the need to give sustenance, sanctuary, training and health care. Strategic gender needs emerge out of an examination of women's subordination and require changes in the structures of sex, class, and race that characterize women's position in any given society. Vital hobbies (strategic needs) incorporate the objective of sex balance.
Development strategies in Uganda ought to consider such angles that sideline women from settling on healthy choices, and draw interventions taking into account the logical components that limit them from taking fundamental insurances in birth control measures. This will result in the reduced population size and the burden of extreme expenditures spent on the over growing population in the country thus resulting in absolute poverty and higher cases of infant, child and maternal mortality rates. In this context, the thesis contributes to a highly relevant, broader discussion on how development should be achieved, and who are the winners and losers of dominant development strategies targeted at societal and human transformation and wellbeing. The study thereby calls upon mainstream perspectives and invites a critical reflection on alternative ways of approaching and rethinking the development of third world countries.
Significance of the research
The study examined the socio-economic factors that influence or determine contraceptive use among rural women in Uganda and especially from Namasuba, Wakiso district. The study also aimed at building on the already existing knowledge on the whole concept of contraceptive use and female reproductive choices, and also the findings would help in developing new approaches for increasing use of contraceptive methods among rural women in Uganda. This may help in the reduction of the ever growing population in the country. This study might also help to fill that existing evidence gap and contribute to literature on the same. Findings from this research may also inform policy makers in rural development on the effective ways of supporting women and men in their daily reproductive life in order to live a safe sexual life.
Apart from providing recommendations on how to improve access and utilization of contraception among the population which is one of the leading causes of poverty in the country, the study also identified the other technologies used by women and why they prefer certain methods of birth control compared to the others. The most benefited category will mostly be government, rural population, women and men, Civil Society Organizations (CSOs), including Non-Government Organizations (NGOs).
Statement of the problem
In Uganda, rural women face a problem of lack of enough support, information, resources and training on how to make healthy reproductive choices, coupled with the negative stereotyping of women as mothers, which leads to questioning of their parenting abilities in terms of family planning and child spacing. The high fertility rate results in high birthrates, bringing about large family sizes with negative impact on the family, the community and nation at large as a result of economic overload in covering the additional demand of the persistent population growth. Access to modern contraceptives encompasses the most important intervention to population management, and thus boosting the nation’s development process.
Limited research has been put in place to address the socioeconomic factors or barriers to contraceptive use among rural women in Uganda. These factors may vary from one society to another due to the gender norms that exist in the different societies as far as use of contraception is concerned. This research helped to bridge the efforts and reality of contraceptive use among rural women in Uganda through identifying the possible factors negating or enabling women’s adoption of contraceptive use. The study also went ahead to find out why rural women don’t access and utilize contraceptives, despite making them available by relevant stake holders and this was done through identifying the major challenges to CU. Hence, the study aimed to understand the access and utilization of contraceptive use among rural women in Uganda, Namasuba village, Wakiso District.
Research objective
The major purpose of this study was to examine the factors influencing access and utilization of contraceptive use among rural women so as to understand the prevalence in use (methods) and constraints experienced by rural women in Namasuba village Wakiso District.
Specific objective
The specific objectives of the study were to:
• Identify the contraceptives accessed and utilized by rural women in Namasuba Village.
• To determine the current use of contraceptive methods among rural women in Namasuba Village.
• To analyze the factors influencing access to and utilization of contraceptive use by rural women.
• To understand the challenges experienced by rural women in accessing and utilizing contraceptives and related coping strategies.
Research question
• What is the prevalence and availability of contraceptives among rural women in Namasuba Village?
• What are the under-lying socio-economic factors influencing the access and utilization of Contraceptive use among rural women in Uganda?
• What other factors influence access and utilization of contraceptive use among rural women?
• What are the challenges faced by rural women in accessing and utilizing of Contraceptive use and how do they cope with the challenges?
• What can be done to enhance access and utilization of Contraceptives by rural women?
Conceptual framework
The major factors identified in the study influence how women respond to birth control methods in the social, cultural and economic context. It should be noted that there are other mediating and enabling factors to contraceptive use that also facilitate its utilization. Respondents are motivated by the reduced costs on some contraceptives like condoms which are provided in some health centers for free which shows how costs of certain contraceptives influence contraceptive uptake and usage (Figure 1).
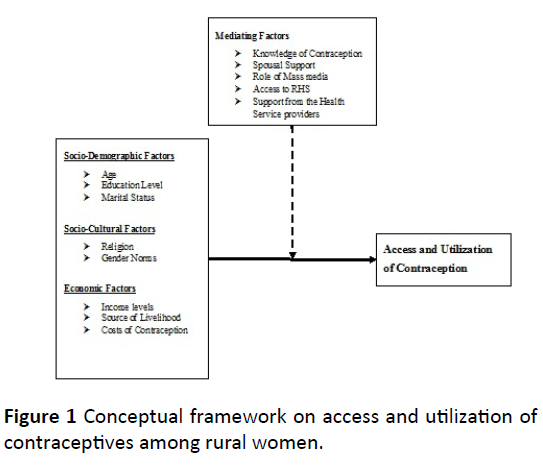
Figure 1: Conceptual framework on access and utilization of contraceptives among rural women.
Research Methodology
The study used a qualitative research design and it mainly used personal interviews which entailed face to face interviews, semi structured questionnaires for rural women, key informant interviews (from the health service providers especially those dealing with reproductive health issues) and informal discussions (for example the use of case stories). However quantitative design was also applied to ensure a larger understanding and interpretation of results obtained from the demographic characteristics of respondents on the factors influencing access and utilization of contraceptive use in Namasuba village.
Research design
The study used a qualitative research design and it mainly used personal interviews which entailed face to face interviews, semi structured questionnaires for rural women, key informant interviews (from the health service providers especially those dealing with reproductive health issues) and informal discussions (for example the use of case stories). However quantitative design was also applied to ensure a larger understanding and interpretation of results obtained from the demographic characteristics of respondents on the factors influencing access and utilization of contraceptive use in Namasuba village.
Area of study
The study was carried out in Namasuba village, Wakiso District. The village is composed of five zones namely, Lufuka, Kalina, Kikajjo, Masajja and Namasuba B. The village is a big area and it’s going through urbanization due to its strategic location close to the main capital city of Kampala. Majority of the people in Namasuba village are traders and business people but a few people practice farming activities mostly for subsistence plus poultry keeping. They mostly deal in agricultural products and the area is known to have one of the biggest periodic markets where people come from far to buy products at a cheaper price. The study couldn’t obtain a clear sample, but Namasuba village has a lot of congestion in settlement, showing the rise in population among the local people. In this case, local services like health centers are put under pressure by the ever growing population and this leaves most of the people unattended to, and provision of basic health services not fulfilled. Other services like education facilities are also in poor shape living people with no education or limited education thus enlarging the illiteracy levels among the local population. This also limits their chances of acquiring knowledge on certain health issues which are partly imparted in Schools. There’s also a problem of early marriages especially among girls because most of them are not in school or any form of employment and are left with no choice but getting married. Therefore, this village was ideal for the study phenomenon because it helped to answer some of the questions under discussion, and limited research is available on rural women and contraceptive use in this area (Figure 2).
Figure 2: Map of Wakiso district.
Study Population
The study population characterized mainly rural women falling under the age of 15-49 years; this was because it is the widely accepted reproductive age of women. The study mainly focused on women in Namasuba village, Wakiso District as the major category, men included as the sole decision makers in a patriarchal society and health workers as key informants. Namasuba village was chosen as a study area because of its ever growing number of rural dwellers and reported cases of teenage pregnancies.
Sample Size and Selection
In order to identify respondents for this study, the researcher used both purposive and snowball sampling techniques for interviews and informal group discussions. Purposive sampling is a type of non-probability sampling which is characterized by the use of judgment and deliberate effort to obtain representative samples by including typical areas or groups in the sample [18]. This sampling technique was used by the researcher to get the hard to reach women and specialized categories, because of the sensitivity of the topic. For this reason, individual respondents were identified through snowball sampling, a sampling method where one respondent identifies another until a sample size is reached or saturated [18]. Snowball sampling was ideal in this research because there was no sample frame from where the researcher could draw a sample of the women using contraceptives in this area to be involved in the study. Data of 85 respondents was analyzed. Rural Women were 55, 10 key informants and 20 male respondents. Key informants were the healthcare providers especially mid-wives and doctors who provide health services to rural women (Table 1).
Table 1: Summary of sampling frame.
| Category |
Sample size |
Sampling technique |
Data type |
Research instrument |
| Rural Women |
55 |
Snowball Sampling |
Primary |
Questionnaire and in depth interviews |
| Men |
20 |
Snowball Sampling |
Primary |
Questionnaire and in depth interviews |
| Health Workers |
10 |
Purposive Sampling |
Secondary/Primary |
In depth interviews |
Data Collection
Data collection took place over a period of a month between 10th July and 10th September, 2017. Before information gathering process, the researcher looked for authorization from the area Local council chairperson (LC.1) to complete the study in the area. The researcher additionally sought for authorization from health workers to take an interest in the study. The information was gathered through narrative investigation or record audit (document review), direct perception and casual talks; researcher administered unstructured polls, key informants meetings and group discussions. Unstructured surveys were used as information gathering instruments during the meetings.
Key informant interviews were likewise used as a wellspring of data for this study. These are subjective top to bottom meetings with individuals who know exceptionally well the community of the study. Key informants were picked purposively in connection to the examination subject. These primarily included health service providers, especially the individuals who gave reproductive health services. Personal interviewing as another data collection strategy included up close and personal collaboration with the respondents and the interview guides were used to gather information from rural women. Report audit/document review was used to gather secondary information from newspapers, diaries, distributed books and expositions. These were used prior and then afterward the field works with a specific end goal to exhibit an adjusted study.
Procedure of Data Collection
In order to recruit primary respondents for interviewing, appointments were made with the relevant respondents. For key informants appointments were made and interviews were carried out immediately because of the tight schedules at the health centers. In-home interviews were conducted and these were also in-depth unstructured interviews to keep the discussions open to participants to gain insights in the target respondent’s culture, preferences and behaviors.
Data Processing and Analysis
The study was purely qualitative and it involved use of case stories, verbatim quotations, narratives and exploration. Qualitative data was analyzed through editing the respondent’s information and this was organized through themes and sub-themes as organized in the objectives of the study. Furthermore Qualitative data was analyzed using content/thematic analysis method. Audio recordings were transcribed verbatim and analyzed using content analysis. Content investigation is an exploration tool used to decide the nearness of specific words or ideas inside of writings or sets of writings. Specialists measure and break down the nearness, implications and connections of such words and ideas, then make inductions about the messages inside of the writings, the writer(s), the group of onlookers, and even the way of life and time of which these are a section [18].
Data was also analyzed using constant comparative method, to synthesize the data. A comparative method was also used to establish between current use and no-use at all among rural women in this village. This was done to get meaningful data of actual use of contraception in this village. Also the researcher utilized data from other interviews like that obtained from the male respondents to corroborate with the findings with other sources.
Research Limitation
The main problem to the study included parts of expenses and subsidizing (Financial Constraints) back to Uganda to gather the relevant information. Subsidizing was an issue to the study because it obliges one to be completely equipped with financial resources, like transport costs keeping in mind the end goal to find rural women. Stationery, for example, a large portion of a ream-of-papers and different materials to use for recording the respondents reactions was additionally an issue. There were parts of some social or cultural silence particularly with the women respondents.
Ethical consideration
The researcher attempted all levels conceivable to maintain the strict moral standards all through the study. All members in the study were legitimately educated about the motivation behind the exploration and affirmation of privacy of their personality and reactions was given. Respondents were not compelled to take an interest in the study and those not willing to take part in the meetings were excluded. Likewise, the respondents were further prompted that they were allowed to stop interest of the study at whatever time they were allowed to. This information was perused out to the respondents from the introductory letter going with the interview guides.
Results and Findings
This chapter presents the data analysis and discussion of the findings from the field study on the socio-economic factors influencing access and utilization of contraceptive use among rural women in Namasuba village, Wakiso district, Uganda. The chapter is organized according to the following themes and sub themes; socio-demographic characteristics of respondents, socio-cultural factors, economic factors and mediating factors influencing contraceptive use, contraceptives accessed and utilized by rural women, factors influencing access and utilization of contraceptives among rural women, challenges experienced, reasons for contraceptive use and coping strategies.
Background information and socio-economic characteristics of the rural women: The demographic and socio-economic characteristics of rural women as primary respondents who were interviewed in the study are discussed in this section. In addition, men were also interviewed as secondary respondents because of their major role in household decision making. This includes age, gender, marital status, education levels, household size and the main sources of livelihood.
Age and gender of respondents
All primary respondents were women in Namasuba village in the three zones of Kalina, Kikajjo and Lufuka because of the nature of the study targeting rural women and contraceptive use. Men were integrated in the study to provide a balanced study and since they are the sole decision makers in the house, their input seemed viable. Figure 3 gives a summary of the age distribution of the respondents (rural women) who participated in the study. Majority of the rural women (34%) interviewed in the study were within the age group of 20-24. This was followed by age groups 25-26 and 30-39 years respectively with 25.5%, the rest 15-19 and 40+ years comprised a 14% in total. Age was a major variable in the study because reproductive matters start from age 15-49 years as the reproductive ages. According to the health workers age is a major criterion followed in determining a suitable contraception or birth control method in matters concerning RH. Therefore respondents below the age of 15 years were not included in the study. The figure below shows the age distribution of respondents (Figure 3).
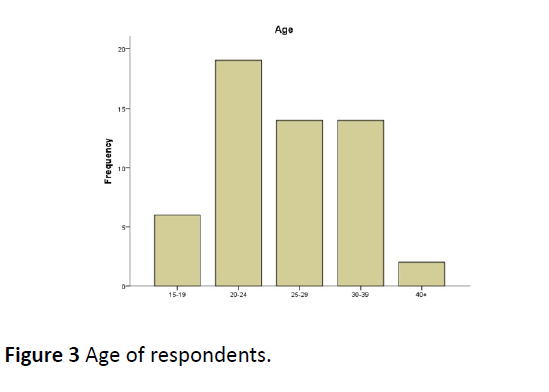
Figure 3: Age of respondents.
Distribution of respondents by marital status
Marital status was also an important variable in determining the factors that influence access and utilization of contraceptive use among rural women in Namasuba Village. Figure 4 above shows the distribution of women in Namasuba village by their marital status who participated in the study.
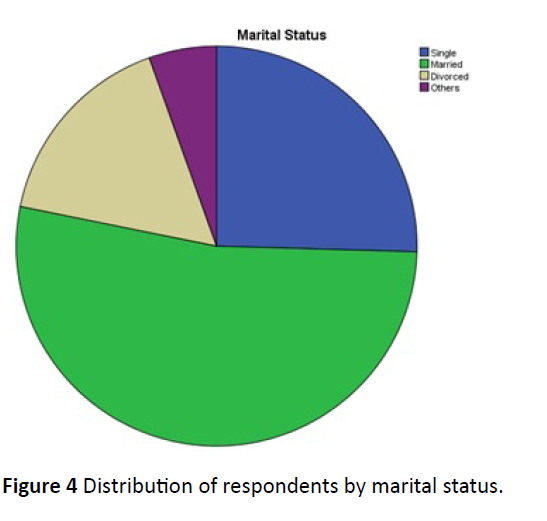
Figure 4: Distribution of respondents by marital status.
Majority (29) representing 52.73% of the respondents reported that they were married. This was followed by 25.45% of rural women (14) who reported that they were single and not in any relationship. 9 women (16.36%) reported to be divorced from their husbands and were running female headed households, the rest 5.45% of the women were either cohabiting or in other trial marriages. As indicated by Nalwadda et al. [19], marital status is one of the real determinants of contraceptive use; unmarried women utilizing contraceptives are defamed and thought to be either prostitutes or unfaithful. Different studies have set up challenges to guarantee contraceptive needs are met in groups where contraceptives are acknowledged to be for married individuals [20].
Education levels of rural women respondents
Results revealed that most women (41.82%) of those leaving in Namasuba village in the three zones had an education level of up to secondary level. The other 20 (36.36%) of the total women interviewed had completed their primary level. The 9 respondents representing 16.36% of the total had no formal schooling background. The last 3 of the respondents representing (5.45%) completed the Uganda Advanced Certificate of Education (UACE). It can be seen that most of the women interviewed did not go further with schooling (Figure 5). Women always face challenges more than the men in education accomplishment. Education among women acts as an empowerment tool to help women demand their rights in matters concerning reproductive health. At the household level there’s still a very big gap in the education of the girl child where most parents prefer to send the boys to school and the girls labeled fit for marriage. This infringes on women/girls right to access to basic education services and which in the end will lead to early marriages with many unwanted and unplanned pregnancies. This situation directly causes a gender disparity in the acquisition of resources and opportunities, as well as gender inequality in household expectations for children’s education; parents have higher expectations for boys’ education than for girls’ [21]. Women with lower education levels are at high dangers of being unable to make sound choice (decisions) both at the community and the family unit level, and this is because of the absence of all defensive riggings provided with fulfillment of Education. During the interviews, a 19 year old married adolescent with two children in Namasuba-Kalina zone agreed to this notion by saying the following in her own words:
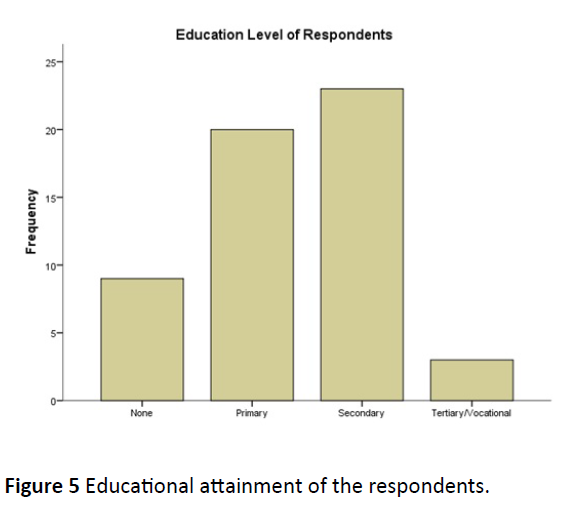
Figure 5: Educational attainment of the respondents.
I quit school when I was in primary three (3) since my parents could not afford to pay school fees for all of us at home. I come from a family of 14 children where 8 of us are girls and the rest are boys. My brothers continued with school because my father believed that they can work and bring money to the home. I was left with the option of marriage since my mother had already seen a man for me. In this way my parents would get bride wealth from me…now I have two children but I can’t even take care of them. I hope and wish that I could go back to school or get skills in tailoring and hairdressing because my dream of learning and speaking English is still alive.
Amid the study interviews with the vast majority of the male respondents (61.03%) had at any rate achieved a training level higher than that of the female respondents. This generally clarifies the discoveries talked about above in proportion of men and women access to formal instruction which for the most part supports the men.
Demographic characteristics of male respondents
This part includes features like age, marital status, educational levels, Religion, prior knowledge to contraception and the types of contraception ever used by the male respondents. The summary of these findings are presented in Table 2 below. According to the study findings, majority of the male respondents (7) were in the age group of 20-24 representing a percentage of (34.67%). This category was seconded by 5 respondents under the age group of 25-29 (24.10%) of the total male respondents. The other respondents in the male category (3) in the age groups 30-39 and 40+ respectively representing 14% of the total population, the rest of the respondents, 2 were under the age group of 15-19. All these respondents were from Namasuba village.
Table 2: Summary of socio-demographic characteristics of male respondents.
| Variable |
Class |
Frequency |
| Age (Years) |
15-19 |
2 |
| 20-24 |
7 |
| 25-29 |
5 |
| 30-39 |
3 |
| 40+ |
3 |
| Marital status |
Single |
5 |
| Married |
12 |
| Divorced |
2 |
| Others |
1 |
| Education level |
None |
4 |
| Primary |
6 |
| Secondary |
8 |
| Tertiary/University |
2 |
| Religion |
Catholic |
8 |
| Pentecost |
4 |
| Islam |
5 |
| Anglican |
3 |
| Knowledge about CU |
Yes |
9 |
| No |
11 |
| Types of contraceptives ever used |
Condoms |
7 |
| Natural Methods |
2 |
| None |
11 |
In terms of prior knowledge about contraceptive use, majority (11) of the male respondents attributed to lack of information concerning contraceptive use. This is either because of lack of enough sensitization on use of contraceptive methods or they are actually not yet well embraced in the community. It should be noted that according to the African home setting, men are the sole bread winners and decision makers in many cases. This implies that lack of enough knowledge on important aspects in family settings may hinder women’s access to and utilization of contraceptive because they lack the support of their spouses. Coupled to the above, the lack of knowledge is also linked to the fact that most men have low levels of education background. It should be taken into consideration that the higher the education attainment of an individual, the higher the chances of contraceptive uptake.
With regard to the use of contraceptive methods, a significant number of male respondents (11) reported not using any contraceptive methods. This was due to reasons ranging religious beliefs, cultural norms and customs and also the lack of awareness on contraceptive availability and accessibility [22]. However, quite a good number of male respondents attributed to use of contraceptives and this can be linked to the cultural and generation shift where men are becoming aware of the value of contraceptives. Men have no readily available contraceptive between the condom, with its high typical-use pregnancy rate and sterilization, with its permanence. Still, using just these two methods, men already account for a third of total contraceptive use in the United States [22].
It is always important to include both men and women in contraceptive use information and knowledge sharing. Men should be put at the forefront because, a woman can, of course control her fertility without her husband’s cooperation, yet when men and women are aware of and responsive to each other’s health needs, they are more likely to obtain necessary services. Data also showed that male respondents who had received some form of education had higher chances of contraceptive use and smaller family sizes as compared to their counterparts who had less education and bigger family sizes.
According to the study findings, it is evident still that religion shapes people’s perception and behavior in most of life decisions. Some male respondents attributed to not using contraception as a result of their religious beliefs and customs that don’t permit them to utilize contraception. In addition, respondents also reported the fear of contracting STDs and above all HIV/AIDS and other STIs and that’s the major reason for use of contraception. In addition, they strongly acknowledged the major reason for CU and uptake so as to be able to give birth to children at the rightful age. This was mostly emphasized by young adolescents who are in their early age and want to delay child birth.
Components of contraceptives used by rural women
Findings in Figure 6 below indicate that most women prefer condoms (35%) and Pills (20%) as a method of birth control during the study. This is mainly due to the fact that condoms and pills are relatively cheaper as compared to the other types of modern contraceptive methods. Condoms and pills are mostly used by the unmarried women and girls who are seeking to control child birth mostly for a short period. Traditional methods (11%) of birth control are also utilized by most women and couples because of their accessibility and availability for most women. Women who use traditional methods acknowledged that traditional herbs of birth control are easy to administer and there’s less stereotyping attached to their access as compared to the other types especially IUDs and Injections (Injecta-Plan).
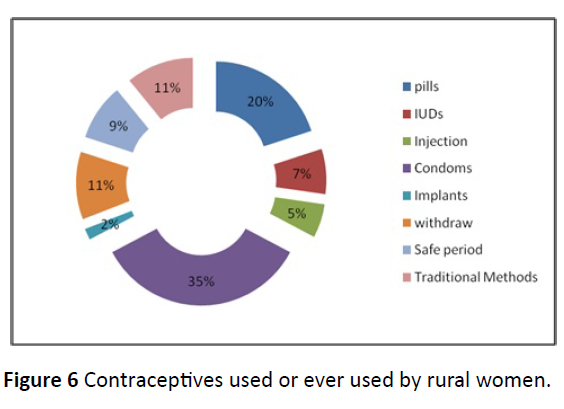
Figure 6: Contraceptives used or ever used by rural women.
Socio-demographic factors influencing access and utilization of contraception
The researcher was interested in finding out the sociodemographic variables that serve as major factors in influencing the access and utilization of contraceptive use among rural women in Namasuba village, in the three zones of Kalina, Kikajjo and Lufuka. The study discovered factors ranging from the age of the respondents as related to contraceptive uptake, the marital status, and the education levels.
Age and contraceptive use
Age is a major factor identified contributing to women uptake of a contraceptive method. Majority of women (9) interviewed who use a contraceptive method fall in the age group 20-24 with a percentage (16.4%) out of the overall 34.5%, the rest of the women in the same age group (18.2%) attributed to not using any contraceptive. Uganda is comprised mainly of young people of 15-24 years of age, 11% of adolescents in Uganda have initiated sex and, 64% of young people have had their first sexual encounter (UDHS, 2006). Young women are thus exposed to the risk of unplanned and unwanted pregnancies for a longer period and as a result in high rates of maternal mortality, unsafe induced abortions leading to death. This therefore calls for an increased need for contraceptive use in terms of birth and fertility control. This was followed by women 25-29 and 30-39 (25.5%). There’s a tie in the contraceptive prevalence rate and uptake in ages 25-39 years because this is where majority of women are able to make responsive decisions of CU and uptake or not to. Young women or adolescents in the age group 15-19 years, attributed to no use of contraception (9.1%) due to reasons varying from age, side effects and cultural norms. The rest 3.6% of women above the age of 40 acknowledged that they are not of child bearing age and are not using any contraception due to their age, not engaging in any sexual behavior and mostly because a desired family size has been achieved. Contraceptive use is lowest among young women, reaches a peak among women in their thirties and declines among older women [23]. This is indicative of a high desire for child bearing among young women and a high growing interest of spacing children among women in their thirties (Table 3).
Table 3: Contraceptive use among rural women by age.
| Age (Years) |
Are you using any CU method? |
Total |
| Yes |
No |
| 15-19 |
1 |
5 |
6 |
| 20-24 |
9 |
10 |
19 |
| 25-29 |
7 |
7 |
14 |
| 30-39 |
6 |
8 |
14 |
| 40+ |
0 |
2 |
2 |
Men were also included in the study as secondary respondents because of their major role in household decision making sand contraceptive use. 20 male respondents were included in the study and 58.6% of the total number of men (12) reported not to use any kind of birth control or CU, falling mainly in the ages 25-29 years. Men’s decision to use a contraceptive method depended mainly on their religious beliefs, cultural norms, educational levels and the gender power relations which put them at an advantage over the women.
Marital status and contraceptive use
Results in Table 4 below show that contraceptive prevalence and utilization is mostly among the married women (15) with a percentage of 27.3% out of all 52.7%. This is mainly due to the fact that contraceptive use is perceived to be used only in the marriage context for issues to do with child spacing and family planning. In any case, it ought to be noticed that, it is in the same establishment (marriage) that most women (14) with a 25.5% not utilizing contraceptives because of elements ranging from social standards, and gender power relations at the family level. In addition some women interviewed attributed to not using modern contraceptives but only traditional methods but these were few. This was also followed by 23.6% of unmarried women (single, 13) who don’t use any form of birth control; unmarried women using contraceptives are stigmatized and perceived to be unfaithful in marriage. Most single young women admitted not using contraceptives due to the societal norms that do not support use of contraceptives at an early age and parent’s disapproval. Parents reject CU because they do not want their unmarried daughters engaging in sexual activity at an early age. Sex before marriage in a traditional context is considered inappropriate and may incur many disciplinary responses from the elders. During one of the informal discussions with a group of young adolescents, one member said the following in her own words:
Table 4: Contraceptive use of women by marital status.
| Marital Status |
Are you using any CU method? |
Total |
| Yes |
No |
| Single |
1 |
13 |
14 |
| Married |
15 |
14 |
29 |
| Divorced |
5 |
4 |
9 |
| Others |
2 |
1 |
3 |
My elder sister got pregnant when she was 15 years old. My parents forced her to marry the man but the man was not yet ready for marriage or any commitment. It really taught me a lesson to use all the protective measures to avoid getting pregnant even if I and my boyfriend were engaging in sexual behavior. We decided to use condoms as our birth control method. I could get them from the youth centre for free and take to him. My mother discovered that I have condoms in my possession, she lost confidence in me. Parents should be made to accept that things are changing and we young people need to protect ourselves not only from pregnancy but also STDs and HIV/AIDS. Many people believe that contraceptives are for the grown up people especially the married.
These findings agree with many studies on factors influencing contraceptive use among women including, Nalwadda et al. [19] and Asiimwe et al. [12] who found out that contraceptives were perceived to be for married couples who have had a number of children. It is noted that young people are stigmatized if they use contraceptives.
Finding in the study also revealed that men have a different perception of contraceptive use, where most of the male counterparts interviewed said they don’t use any contraceptive method. One male respondent (married) said the following during the interviews when asked of his perception on contraceptive use in his own words:
My name is Muwanguzi David (gave permission to be mentioned) am a gate keeper at a secondary school in Namasuba-Kikajjo zone. I spend most of the time sitting here at the gate and not going anywhere to look for women. I have my wife who is always waiting for me at home and I trust her not to cheat on me. I don’t see any reason why a person can use those things you call contraceptives, because I trust my wife and she trusts me too. I have to enjoy my sex life with my wife without any obstacles like condoms, and I also want to produce more children until Jesus comes back.
Education levels and contraceptive use
Female education appears to be an important determinant of modern contraceptive use, the more a woman is educated the more likely to make choices on child birth and mostly the use of all reproductive health technologies including contraception. Cohen reported that small amounts of education have been found to sometimes rise rather than lower fertility because it breaks down traditional birth spacing practices such as prolonged breastfeeding or postpartum abstinence without lowering fertility desires or increasing age at marriage. Table 5 below illustrates the field findings which are related to others study findings.
Table 5: Contraceptive utilization by levels of education.
| Education Levels |
Are you using any CU method? |
Total |
| Yes |
No |
| None |
2 |
7 |
9 |
| Primary |
10 |
10 |
20 |
| Secondary |
10 |
13 |
23 |
| Tertiary/Vocational |
1 |
2 |
3 |
Findings in Table 5 reveal that use of contraceptive methods among those in Primary (18.2%) and Secondary (18.2%) education was higher than those who had no education background (3.6%). The last category (1.8%) indicates a less desire to use contraception due to the age variable. There is a significant association between contraceptive methods and level of education. It should be noted however that the number of non-contraceptive users exceeds the ones using contraceptives by levels of education. Majority (23.6%) of the female respondents reported not to be using any modern contraceptive method per the overall total of 41.8%. These had an education level of up to secondary, choices at this level depend mostly on the household level of autonomy where by most women at this level have to consult their husbands on matters concerning child birth and use of contraception. Most women in this category are married or in a defined relationship as those women who dropped from primary level (18.2%).
The study also revealed that a husband’s education is likely to increase the likelihood of a woman using contraceptive method as divergent to lowering it. A few men included in the study with some education acknowledged the use of contraception and in fact helping their wives in accessing them in order to plan and space their children. During an informal discussion with male respondents, one respondent 29 years, married in his words said:
It’s not always that men don’t want to use contraceptives. Sometimes I ask my wife to use the IUD for longer child spacing so that we avoid frequent births like a rabbit…in this era of absolute poverty we may not manage a large family size so the only way to do so is limit on the number of children we give birth to. But this is most common in men who have attained a certain level of education; other men will tell you they don’t want like most of my friends here in the village.
Socio-cultural factors influencing access and utilization of contraception
The researcher was interested in finding out the sociocultural factors influencing the access and utilization of contraceptive use among rural women in Namasuba village, in the three zones of Kalina, Kikajjo and Lufuka. The study discovered factors ranging from religion and gender norms, (beliefs and practices and community networks and attitudes).
Religion
The study revealed that majority of rural women (18) was from the catholic and Islamic faith with the same representation of 32.7%. Of all the women in the catholic and Islamic faith, 20.0% and 9.1% acknowledged no use of contraception due to their religious beliefs. The rest of the respondents were from the Anglican (18.2%) and Pentecost (16.4%) or born again faiths. Religion in Uganda plays a very vital role in the decision of the people since the country is built on a religious background. People perceive religious teachings of great importance, and in most cases these teachings are against CU (Table 6).
Table 6: Contraceptive use by rural women by religion.
| Religious Affiliation |
Are you using any CU method? |
Total |
| Yes |
No |
| Catholic |
7 |
11 |
18 |
| Anglican |
5 |
5 |
10 |
| Islam |
8 |
10 |
18 |
| Pentecost |
3 |
6 |
9 |
Many women in Namasuba village acknowledged there use of contraception as based on the doctrines of their respective faiths. During the interview one male respondent argued in his words:
Usually it’s not safe to go beyond the words of Allah; the Quran emphasizes giving birth to children because they are considered to be gifts from Allah. The Imam at the mosque is totally against these family planning methods and this is a big sin which awaits punishment. That is why Islam permits the provision of extra wives in order to give birth. Children are even a source of labor in the old age. If you give birth to only one child or two and they unfortunately die what would you do? It is always good to have backup when the others die. As for me I think the people should be left to produce as it was long time ago during our great grandfathers and see whether they will starve (Married man 38 years).
This shows a clear picture of how religious beliefs shape people’s behavior and knowledge of certain aspects of life including matters pertaining reproductive health and especially contraceptive use. Some women respondents especially from the catholic faith quoted the book of Genesis in the bible saying that “go multiply and fill the world…” as commandment to mankind by God which has to be respected until when Jesus comes back. In addition to the above, the catholic women who use contraceptives in most cases received some awareness either with educational attainment or through sensitizations and health talks.
Gender norms
Gender is also another detriment of contraceptive uptake among women in Namasuba village. This is because society in Uganda is organized in a set of norms and beliefs that shape the way women and men perceive certain aspects in life. These norms are normally socially or culturally constructed during the process of socialization, and mostly put females at a position of passiveness as compared to their male counterparts. The study found out many power relations in terms of decision making in choices concerning contraceptive usage. Women are socialized to be submissive to their husbands in matters concerning sexuality and they reported so many hindrances from the men in matters concerning child birth. This is because a woman’s role in marriage is shaped in child birth without any birth controls. Most women interviewed recalled spousal disapproval on matters concerning contraceptive use to an extent of being divorced or abandoned and labeled promiscuous because of refusing to give so many children as society wants to. During the informal discussions one female respondent lamented her case in her own words:
My name is Cecilia Nassiwa (agreed to mention name) am 28 years old. I am married with 4 children, I have been married with my husband and everything was going on well until not long ago when we had this last born that things became worse to the extent of divorcing me. I have been secretly using contraceptives (pills) in order to avoid unwanted pregnancies and child spacing as educated by the doctors, but time came when I had to stop doing it in secret and tell my husband about it because he is the head of the house and makes all the decisions. When he came back home I told him about the need to start using contraceptives to space children because we still had the desire to continue giving birth to children. He was so furious, he bit me up like a child, blamed me of wanting to sleep with other men for fear of becoming pregnant and other things. He said he will divorce me if I ever talked about using contraceptives. I have no problem in using pills because they reduce on my burden as a woman on continued pregnancy and to take care of myself to but I have to listen to my husband for fear of divorce and living my children in the hands of other women he might get (married woman, 28 years).
The above notion corresponds with Laurie and Alex [24] using data from the UDHS, 2006 discovered that women in areas or societies where females more commonly have control over household decisions were 29% more likely to adapt or use modern contraceptives. This is because communication on matters concerning when and how to give birth to children is communicated freely between the couples without fear of the unnecessary outcomes. These are mainly in the urban areas were services are readily available to the people and education attainment has been achieved to a certain minimum level for safe RH choices. In general, individual’s decisions and choices are shaped by the perceived beliefs and norms of the community on matters concerning CU.
Economic factors influencing access and utilization of contraception
The study aimed to assess the economic factors that influence women’s access to contraception in Namasuba Village. This was done to inform the study whether economic conditions have an effect on women’s contraceptive choices and uptake. Economic factors are arranged varying from sources of livelihood (to determine the income levels), employment status and the costs of contraception.
Source of livelihood for women in Namasuba village
The researcher was interested to find out from the women and men in the study the other sources of livelihood they engage in, in order to make health choices and take care of their families. This was mainly because aspects of a large family size among couples whether married or unmarried but with children require a decent and earning job or career to be able to provide the necessary basic necessities of life to the beneficiaries of the household especially children with gears and safety nets like basic health and education and also a mother’s wellbeing. Table 7 above shows the frequency distribution of rural women in Namasuba village according to the sources of livelihoods engaged in both formal and informal to raise incomes.
Table 7: Sources of livelihood for respondents.
| Source of livelihood |
Number of rural women |
| Cashier |
1 |
| Cleaner |
1 |
| Commercial sex worker |
1 |
| Farming |
7 |
| Hairdressing and saloon |
3 |
| Laundry services |
1 |
| Charcoal selling |
1 |
| None |
18 |
| Sells soft drinks |
1 |
| Operates a restaurant |
1 |
| Shop attendant |
1 |
| Selling clothes |
1 |
| Selling airtime |
1 |
| Selling vegetables |
4 |
| Housemaid |
4 |
| Student |
1 |
| Community worker |
1 |
| Office attendant |
1 |
This information (as shown in the table above) shows that majority of the respondents have no sources of livelihood to help them earn a certain income for the basic necessities of life. Those who have a means of livelihood are confined in the informal sector which provides fewer alternatives to development in terms of providing health choices to RH and CU. Most families interviewed in the study had a large number of living dependents with an average number of 5-10 children per woman. This indicates that most of the little resources obtained from the petty jobs done by women and their spouses are diverted to take care of the family and less is shifted to the health of the mothers themselves. This seems to be a household level problem but it puts more strain on the national health system and retards the development process.
In addition, the study was also interested in finding out the status of employment for rural women in Namasuba village. Findings from the study indicate that most women are unemployed (49.09%) with no form of formal or informal employment. Employability status is an important factor in influencing maternal and child care service utilization in collaboration with contraceptive utilization and uptake. Findings from the study shows that majority of women (27) out of the total sample interviewed were unemployed making it difficult for them to access the market for contraception and demand for them is limited. The employment status of women has also been linked to knowledge and use of contraception. Women (25.45%) who work in the public sphere have a higher rate of use of contraception compared to women who are confined in the domestic sphere (mostly the unemployed). Health workers also add that paid work or self-employment provides an alternative to self-development for women, through provision of satisfaction in child bearing and rearing. Women can be in position to take care of them and their children from the incomes obtained from their work. There’s limited number of farmers in Namasuba village because the place if semi-urban heading to urbanization through population increase but limited healthcare services.
Costs of contraceptives
The study assessed the costs of various contraceptives available to the women and men in Namasuba village. The costs involved in the buying and utilization of these contraceptives is an aspect that can be overseen but contributes primarily to women inability to utilize the available contraceptives. According to the health workers condoms and pills are utilized more because they cost less between 500-1000 and 1000-5000 Uganda shilling a packet respectively. They are mostly utilized by the unmarried, who haven’t started child birth. Married women use the long term methods of birth control which are extremely expensive to the low income earners or women who have no income at all. Injector plan (or the injection) costs 3000-10,000 shs (Uganda shillings) for 3 months, whereas the Intra-Uterine Device (IUD) costs between 50,000-80,000 shs (Uganda shillings). These costs are too expensive for most women, as one woman narrates during the interview in her own words:
Some women agree on use of contraceptives with their partners but the problem is these contraceptives come with a cost. It is always too expensive to get most of them especially the injection which is short term for a period of only three months and the money to buy it some women can’t afford in the same period due to so many being unemployed and depending on husband’s money which is not enough. Women would have been able to access these contraceptives if they had like good paying jobs to raise some money to be able to pay for them depending on what they use…you have to also consider the transport to go to town, you may end up not using these contraceptives and getting pregnant(Unmarried woman, 26 years).
Mediating factors to contraceptive use by rural women
As a precursor to understanding the contraceptive choices and factors driving their uptake among rural women in Namasuba village, the study investigated the mediating factors that serve as a linkage between women’s choices in CU and Reproductive Health. In this part, mediating factors include; knowledge of contraception, role of the media, spousal support, access to the health services and support from the health service providers.
Knowledge of contraception
Most women attributed to the fact that they have ever heard about contraceptive use through different platforms like radios, hospitals, billboards, through community health dialogues and health surveys from the health centers. However a group of young adolescent girls said the lack of enough family planning and contraceptive choices was associated to their not using contraception. During the interviews, most women and girls first heard information during their first visits to the hospitals and also over the media (radios), so this information is missed to the women who can’t afford health care systems. Women with disabilities face major challenges in access health centers because of their physical limitations and lack crucial information on matters concerning reproductive health and especially CU.
Views from personal interviews revealed that radios helped in the acquisition of knowledge and information on contraception, through adverts and open discussions on health issues in addition to providing a forum for sharing personal experiences thus helping to reduce on ignorance about reproductive health issues among rural women. Rural women who do not have access to radios and or televisions could lack access to vital information such as the use of condoms and pills that would help guarantee them safely against unwanted or unintended pregnancies, and to live a safe sex life. It is through radios and televisions that people are easily and mostly informed in this era. Health workers also emphasized that due to the fact that most health centers are located far from the residents and the most convenient means to access this information is over the radios.
It should be noted, though women had positive information and knowledge about contraceptive use, quite a good proportion of women reported not using contraception because of the negative information got from their friends about their experience in contraceptive use. During one of the interviews a female respondent aged 23 years narrates her knowledge on contraception:
When I was still in school, I had friends who were already sexually active. They used to sneak out of school and go to clubs and play sex with men but they used to use condoms. They used to say after using the condoms; they could itch down in their genitals or vagina. So whenever I could remember their stories I could be puzzled on which method to use. The doctor advised me to use the female condom but it’s too big for me. I want to avoid unwanted pregnancies and sexually transmitted diseases but problem is when you hear about people’s stories, I get scared.
The story above indicates that some women have the desire to use contraception but negative myths or misconceptions exist on CU. Health workers say that most women are reluctant to go to the hospital for this kind of information and that’s why health centers have developed a strategy to extend the community outreaches to the people. Women’s health is also subjective both by biology and by cultural institutions which define power relations within households and between men and women, and influence women’s access to knowledge and resources.
Therefore, access to information and ownership of knowledge and information are major key issues in women’s access to health care services. Unmet needs for CU are mostly influenced by these issues in the long run.
Spousal support
Support from spouses has been identified from the study as a major pre determinant of contraceptive uptake especially among women. This is because women require certain form of approval from their husbands on whether or not to use contraceptives in a marital relationship. It has also been identified in most young female adolescents interviewed that it’s always a boy/man who brings a condom when going for sexual intercourse. In this case the support of the spouse enables a woman to use a certain method of birth control and the reverse is true for those couples where the man is not in agreement.
Most women who come to access these contraceptives first seek permission from their husbands. As you see our society is rooted in patriarchal values that put man in a decision making position than a woman, so it is always hard for her to make any move without approval of the husband. In cases where women don’t ask or talk to their husbands on contraceptive use, situations of family break ups and domestic violence prevails Midwife, St. Apollo Kivebulaya Namasuba Health Centre.
The findings above indicate that men’s control over women’s reproductive health and sexuality is likely a result of upstream factors related to the masculinity and gender role norms prevailing in most patriarchal societies. In addition, issues to do with sexuality, fertility and a large family size are strongly linked to the definition of man-hood in many rural areas in Uganda.
Access to health service systems
Accessibility to health services including hospitals and clinics involves aspects of geographical location and costs involved to reach the service systems. Majority (47.69%) of women respondents reported in access to health care systems as a major hindrance to contraceptive use. This is because the village is so over populated and there’s only one government aided hospital to handle the growing number of people in the area. Most private clinics reached to in the study offer services related to contraceptive use at a much higher price compared to the governments’ hospitals. There’s also a problem of shortage of drugs and contraceptives in these hospitals, since health workers get them at a cost. During the interview with a doctor, he said in his words:
In most cases we also buy these contraceptives at an expensive price, so there’s no way we can give them out to all the women in the village. We fix the price of the contraceptive according to the price bought and also following the Ministry of Health (MOH) regulations. This is where I call upon the government to help the grass root clinics and pharmacies that provide these services through equipping them with more contraceptives. This will in the end improve the livelihood of the general population and reduce on the cases of maternal mortality, infant and child mortality and so many unhealthy abortions leading to death and so many adverse effects.
In addition, Mathole et al. [25] found poor quality of care services and the negative attitudes of the health service providers as barriers to utilization of contraceptives and Antenatal Care (ANC) in Zimbabwe. They study highlighted that poor relationships between the doctor and the patients, and the unfriendly environment were the major reasons some women preferred not to go to hospitals and to adopt to traditional methods of birth control. Youth friendly or adolescent friendly services are encouraged in this case to attract more girls to adapt to utilization and to avoid unintended or unwanted pregnancies.
Reasons for and against contraceptive use
The study examined the reasons why some women and men use contraceptives while others don’t. During the study interviews, women and men combined gave reasons as to why they decide to use a certain contraceptive method and actually not to, and these reasons are explained below.
According to the study findings, it is evident still that religion shapes people’s perception and behavior in most of life decisions. Majority male and female respondents attributed to not using contraception as a result of their religious beliefs and customs that don’t permit them to utilize contraception. In addition, respondents also reported the fear of contracting STDs and above all HIV/AIDS and other STIs and that’s the major reason for use of contraception. Women strongly acknowledged the major reason for CU and uptake so as to be able to give birth to children at the rightful age. This was mostly emphasized by young adolescents who are in their early age and want to delay child birth.
Unintended/unwanted pregnancies are one of the leading causes of maternal mortality among most women in Uganda. Respondents pointed out that the use of condoms and pills help them most in the prevention of unwanted pregnancies and other STDs/STIs. This is because they are easily used and readily available in the hospitals and shops as compared to other methods. Unsafe abortions occur on a daily basis among women, and these lead to death because they are not done in the right way. This is because abortion is illegal in Uganda and highly punished if carried out.
According to the findings in Figure 7 above, the major reasons against contraceptive uptake among rural women in Uganda are related to the so many side effects (8) associated with the birth control technologies. Some women (6) also pointed out the fact that their religious beliefs and background doesn’t permit them to utilize contraception. This is mainly according to the catholic and Islamic faiths. Non-use of contraception varies from individual to individual as there are some women who reported not interested in the use of birth control methods. It should be noted that 4 women reported using traditional methods of birth control and these include but not limited to use of local herbs and others.
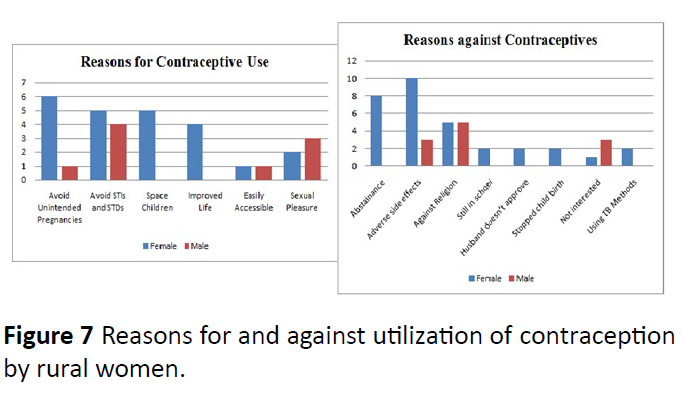
Figure 7: Reasons for and against utilization of contraception by rural women.
Challenges faced by women in access and utilization of contraception
User perspective: Some contraceptives come with negative effects on women's health which discourages them from using them for example missing their monthly periods, and other diseases like cancer of the reproductive system. It should be noted that this was the major challenge listed by women as a major challenge to contraceptive use. Some women gain a lot of weight (over weight), headache, bleeding, loss of sexual appetite, making them dry. During interview with a midwife she added to these findings as below in her own words:
Among other side effects, most women say they become fat, others thin. Some become black and others brown, some women experience over bleeding, and or missing their monthly periods. In addition some women say they lose appetite for food and sexual pleasure when they use contraception. Women are affected differently from each other and it mostly depends on the type one uses. However much as most women experience a lot of side effects, they also acknowledge the advantage of spacing children, reducing on abortion cases among women, good feeding and being able to pay for the education of their children with the help of CU in birth control. (Midwife, Lufuka Nursing Home).
Essential services for reproductive health are mostly provided in urban areas and cities whereby most women find it hard to obtain the transport costs to these health centers which are mostly government aided and providing services at a cheaper price. This therefore limits their utilization of contraceptive methods and contributes greatly to the growing population in the rural areas of Uganda, because of the uneven distribution of these health services.
Wrong information or unhealthy education talks from the community through negative attitudes towards the use of contraceptives and the misconception on their use. Women have a fear in them to ask for contraceptives because of what they hear from their networks in the communities which are mostly against the use of contraception, mostly myths and norms that are against contraceptive use.
Religious beliefs especially Catholics and Islam that are against the use of contraception and family planning methods were also identified as major challenges to CU and uptake. Problems at the household level where men refuse women to adopt the use of contraception.
Health service provider’s perspective: Traditional methods of birth control which have been adopted by women but are not effective enough to control fertility. This is because most women are still confined in their traditional beliefs and methods and some shun the modern methods of birth control with so many misconceptions.
Lack of income and resources to cater for the reproductive health of rural women; since most women are unemployed, it becomes difficult for them to access reproductive technologies or contraception since most of them are for sale on the market. It should also be noted that most women lack financial support from their husbands thus posing a major challenge to their access and utilization of Contraceptive use. One doctor at a health Centre in Namasuba noted that in his own words “Financial problems are the major challenges for these women, some contraceptives are way too expensive like the injector plant and yet most women can't afford it”. These words from the health service provider actually correspond to the researcher’s views from the study as portrayed in Figures 4-6 above. Most women lack decent formal jobs that can help them gain income to take care of themselves and their families.
Poor health literacy is also another leading challenge in the access and utilization of contraception among most women. Health literacy is the degree to which patients understand basic health information such as following instructions from a health care provider, managing a chronic illness, or taking medication properly. Rural residents especially women and men are at risk for low health literacy because they have lower educational levels as compared to residents of metropolitan areas. Low health literacy is a particular problem for people in poverty and people with limited education or English proficiency. This thus affects their access to basic family planning services because of the limited knowledge on how to use the services.
How rural women cope with the challenges
The study was also interested in knowing how rural women cope with the challenges they mentioned in order to improve access and utilization of CU. Rural women did mention a few ways in which they cope with the challenges they face which are explained as below:
Women have tried to change the negative attitudes of the society towards them. This they have done through advocacy towards the promotion of their fundamental rights as women. These rights are clearly stated in the Constitution of Uganda (Article 33 and 35) respectively and other international documents like the Universal Declaration of Human Rights (UDHR) among other Human Rights documents.
Women in Namasuba village have formed informal groups (social support) in order to help raise some money in order to access reproductive health services. These groups are mainly formed by women inform of SACCOs and it came to the researcher’s knowledge that they are sometimes supported by their networks for them to continue existing. In this way, they can be able to support themselves and their friends in the networks to raise some money in case of emergencies like sickness and childbirth. Each member in the group has to contribute 1000 UGX (0.31 USD) per week in order to keep money in the treasury and distributed weekly according to who is to receive that particular week.
Women in this area have also urged doctors to reduce on the content of the medication in the contraceptives in order to reduce on the so many side effects among others related to over bleeding. Doctors take a clear criterion in selecting a suitable method for these women through the health history examination.
Strategies to improve contraceptive use from the existing policies
Uganda battles to address one of the most high fertility rates on the globe. According to Marie Stopes International (MSI) strategic paper in 2009, the unsuitably high rate of unmet requirement for family planning (41%) plainly demonstrates the requirement for enhanced and extended programmatic development in underserved areas. Within this context, greater contributions have been made to ensure that modern contraceptive use in Uganda show targeted outreach and social marketing initiatives which have had a direct impact on shifting fertility rates, and modern contraceptive use in the desired directions. Specifically, by giving lasting family planning techniques beyond static centers and taking services into rural, hard-to-reach regions. It should be noted that NGOs are playing a vital role to enhance provision of family planning methods to the people although the pace is still slowed down by the traditional society norms and customs.
In October 2004, Uganda endorsed its first extensive National Adolescent Health Policy. In a nation where more than 50 percent of women are sexually active by age 17, the endorsement and usage of such a strategy was basic to enhancing the RH of young people [26]. A number of CSOs including NGOs have played a basic role in the accomplishment of RH strategies and programs at the grass root level especially in the rural areas which toiled for a long time to pick up endorsement for the approach. However, the decentralization of power and obligation regarding RH has displayed new difficulties to completing arrangements and securing assets at the area level and beneath, where existing limit is frail. Likewise, destructive conventional practices, for example, limitations on spouse legacy and sexual orientation segregation, frustrate the execution of key strategies [27,28].
Above figures shows some data from the health center outreach activities to extend services to the people. During the outreach sessions, health workers are also informed of the issues that the clients can’t afford to say at the health centers due to accessibility and affordability issues in matters concerning contraceptive use and uptake.
Health workers in Namasuba village deliver reproductive health services including contraception following the RH policies and strategies that help them to reach out to different men and women though the process is still slow due to the fact that these technologies have not been embraced by the people [29].
In order to reach out to clients, we organize community health talks on matters concerning reproductive health. During these talks, we carry out condom distribution and demonstration and always encourage the people to visit the health centre for more information about the availability of other methods of birth control. This strategy is gaining momentum and has helped the hospital know which method is more desired by the people compared to the others. This is done through keeping records of the technologies that are distributed out and later we know which works best. Health Service Provider, Namasuba Village [30].
In addition to community identification and registration of clients in the villages, another strategy to reaching out to people is through massive sensitization of the masses through media campaigns, provision of IEC (Information, Education and Communication) materials and community educative health talks. This is also another strategy to ensure access and utilization of contraception among rural women in Namasuba village.
In addition, during our outreaches we do blood testing among women before they start using contraceptives especially in family planning. It will help women adapt to methods that are compatible with their bodies and hence minimize of all the side effects. Community sensitization through outreaches, community dialogues in form of health service provisioning to see what the people want and also form support organizations to extend services closer to the people, Community Outreach Officer, Namasuba Village.
The health center normally sensitizes both men and women about contraceptive use, however in most cases men don't want to attend these trainings because they believe it’s a woman thing. According to health service providers, Counseling is also done among men and women as a way to improve access to contraception through encouraging them to have small number of children. In addition, Health education and advice, management of side effects, investigations and follow-ups of clients is also ensured as a way to maintain proper utilization of contraception. Rural women first receive counseling, if they accept the methods; they are examined according to their health history and bodies to ensure a suitable method [31-36].
How the strategies have helped rural women
Women have gained knowledge on contraceptive use and the access rate has improved. According to health service providers in Namasuba village, the numbers of women accessing and utilizing contraception has increased over the past few years. Actual numbers at the time of the study wasn’t available on how many women access on a daily basis but according to health workers acknowledge great improvement [37].
Registration of success stories from some women who have succeeded through use of contraceptives. The health workers acknowledged that there have been quite a good number of success stories where women and men’s lives have changed drastically after the implementation of family planning strategies. In addition, couples are now able to plan for their families and decide on when and how to have children.
Women have been empowered in the long run and they can choose methods based on their choices and wisely through the support of health care service providers [38].
Discussion
This chapter presents the summary, conclusions and recommendations of the study. The major aim of the study was to analyze the access and utilization of Contraceptive use among rural women in Namasuba Village.
Summary of major findings
The major purpose of this study was to explore the factors influencing access and utilization of contraceptive use among rural women so as to understand the prevalence in use (methods) and constraints experienced by rural women in Namasuba village Wakiso District. Data of 85 respondents was analyzed. Fifty five rural women were interviewed, coupled with 20 male respondents and 10 key informants. Key informants were the healthcare providers especially mid-wives and doctors who provide health services to rural women. The study was mostly qualitative but quantitative methods were borrowed to determine the prevalence in use of contraceptive methods. Data collection methods included personal interviews and key informant interviews which were unstructured, and document reviews [39-41].
The study findings revealed that various social and economic factors can influence women’s access to Contraception. This implies that negative circumstances that impede access to information as a result from the above are not favorable for rural women to CU. These circumstances may include discrimination or stereotyping, isolation and denial of information on the availability of contraception provided on the market. These results further reveal that rural women, who had knowledge about contraceptives and their usage, utilized such knowledge to care for themselves and living a safe sex life. Women who had less or no prior knowledge about contraceptives and their use were at a risk of poor family planning methods, lack of child spacing and other risky STDs above all HIV/AIDS. The study also found out that the use of condoms and pills were the leading methods of contraception known by majority women and men. This was under the pretext that these methods were the most advertised and talked about by the public. In addition, condoms and pills were considered more easily accessible and difficult to run out of stock from pharmacies or hospitals. Some respondents also acknowledged that condoms and pills were easy to use with fewer complications as compared to the other methods of birth control. It should be noted that some rural women interviewed preferred the Traditional methods provided by TBA because they are easy to administer and culturally accepted [42-47].
Findings also revealed that rural women face some challenges in the access and utilization of CU. These challenges include, lack of information and knowledge about CU, negative cultural (religion) and gender norms of the society towards women use of contraception, low levels of income (poverty), illiteracy (in form of low levels of education attainment) and language barriers, unfriendly reproductive health service systems and care providers, and cost factors, like costs of contraception and transport costs to the health centers. Thus the study observed that there was a great need to address some of these aspects. Most importantly, there was need to change the negative cultural and religious attitudes of the society towards women utilization of CU, sensitization in order to create awareness on issues concerning CU. Extension of RH services to women in order to create proper utilization of CU, spousal support and the provision of contraceptives free of charge to women. Key informants also identified some of the challenges which they face in the delivery of contraception to rural women which include traditional beliefs, finances, accessibility which is limited by transport means and costs of CU, ignorance about RH issues by women, illiteracy and low self-esteem by some women [48-50].
Relevance to development theory
Constituting the largest part of Uganda’s population, rural households are a highly important group of society. The development of the country is mainly measured by people’s wellbeing and mostly in terms of health issues. Empowerment of women mainly encompasses giving them the necessary gears to facilitate their own self development and that of their families since they are the family care takers, through educating them on limited fertility measures with husbands or men at the fore front [51].
Development strategies in Uganda should consider such aspects that sideline women from making healthy decisions, and draw interventions based on the contextual factors that limit them from taking necessary precautions in birth control. This will result in the reduced population size and the burden or extreme expenditures spent on the over growing population in the country thus resulting in absolute poverty and higher cases of infant, child and maternal mortality rates [52-58]. In this context, the thesis contributes to a highly relevant, broader discussion on how development should be achieved, and who are the winners and losers of dominant development strategies targeted at societal and human transformation and wellbeing. The study thereby interrogates mainstream perspectives and invites a critical reflection on alternative ways of approaching development.
Economic development mainly encompasses aspects of fertility control in order to boost the country’s economic growth. This is to a greater extent due to over population growth rates that mostly result into social and economic problems which may retard the development process. This therefore means that the idea of development should take into consideration fertility reduction especially in the developing countries not forgetting the aspects of gender equality in fertility and sexuality control. This is because women are affected differently from the men in matters concerning fertility and childbirth. In most cases women’s sexuality is controlled by the man and this is mainly because if the societal structure of putting men at a more privileged position as compared to the women [59-61].
Conclusion
The study findings revealed that various social and economic factors can influence women’s access to contraception. This implies that negative circumstances that impede access to information as a result from the above are not favorable for rural women to CU. These circumstances may include discrimination or stereotyping, isolation and denial of information on the availability of contraception provided on the market. These results further revealed that rural women, who had knowledge about contraceptives and their usage, utilized such knowledge to care for themselves and living a safe sex life. Women who had less or no prior knowledge about contraceptives and their use were at a risk of poor family planning methods, lack of child spacing and other risky STDs above all HIV/AIDS.
The findings indicate that certain variables like lack of spousal support and lack of immediate knowledge on contraceptive use affect the decision to seek health services care and attention in matters concerning reproductive health and these are mainly socially and economically constructed. This sociological view of the problem at hand should help to influence policy and how policy makers can find solutions to address the adverse effects that can emerge from the identified factors in the short and long run. These findings are consistent with the literature and suggest that the poor people and especially those living in the rural areas have access problems relative to those who can actually afford to access these services.
Therefore, policy makers should use bottom to top approach in the provision of services especially contraception to rural women since they know better the problems affecting them in matters concerning reproductive health and also ensure community involvement towards improving access and utilization of contraception among rural women, this would help reduce the negative attitudes attached to women access to CU and will create a conducive environment for them.
Another alternative could be to lessen the prices attached to these services so as to ensure utilization of contraception. This is because in the long run it’s the government highly affected by the uncontrolled growing population with no basic service provisioning. The number of children should at least be reduced to 4 children per family as per now and concentrate on addressing the effects already caused by the population increase.
The study achieved all its objectives. Concerning the general objective which was to analyze the access and utilization of CU among rural women, with the view of examining the socioeconomic factors and the challenges faced by rural women in access to and utilization of CU, the following were achieved. Many factors influencing the access and utilization of CU among rural women were identified and these included the age, religion, marital status, employment and income levels, role of the media (information), gender and cultural norms and attitude of the communality towards women’s use of contraception. Gender power relations in the home where women are subordinated most by their husbands in terms of sexuality and RH were also identified. Affordability in terms of incomes and resources, discrimination and isolation, accessibility in terms of transport and the long distances to health centers.
Respondents suggested possible ways in order to improve access and utilization of CU which included; contraceptives to be provided free of charge to them, extend services of reproductive health closer to them, change of the negative attitudes towards CU, access to information concerning reproductive health and especially CU, effective and affordable methods of family planning (contraception). Key informants called upon government to increase awareness and sensitization of CU in order to reduce to the increasing population and also to reduce costs in accessing the contraception.
Recommendations
Basing on the preceding discussion of the findings and in particular the possible ways to improve access and utilization of CU among rural women, certain recommendations were advanced by the researcher and the health care providers, which include:
Health workers
There’s need for greater understanding by the health service providers and policy makers of the influences underpinning societal attitudes towards sexuality and contraceptive use in this setting, and more extensive communication between health care staff and women would facilitate positive action towards improving safe motherhood and reproductive health services for rural women and reduce cases of unsafe abortions, unintended or unwanted pregnancies, in addition to reducing HIV/AIDS.
Additional research should address the gaps in knowledge about the reproductive health care needs such as the unmet need for contraception for these rural women. Majority women need greater education and sensitization on reproductive health and improved access to health care. This can be done in the form of trainings, advocacy and lobbying in order to improve access and utilization.
There should also be special delivery of reproductive health services especially contraceptives to women with disabilities especially to the lame, and blind women. This will create easy access and utilization of reproductive health technologies.
Lastly, women’s effective access to health care involves the interrelationship of many complex factors. This can only be assured if health services are considered available, affordable, appropriate and acceptable by women especially in the rural areas, since they are greatly affected by the negative effects that come as a result of the above.
Government
There’s need for improvement in rural health service systems through providing the necessary equipment’s in the health centers. In addition more public hospitals should be built in the rural areas to address the issues of inaccessibility and transport costs to the urban centers by rural women.
The Government of Uganda should endeavor to equip rural health service centers with necessary RH services. This is turn will help to address the problems of lack of availability of certain services when need by rural women.
Economic empowerment for rural women and men is also a fundamental basic requirement for improve in rural women and men’s livelihood. Rural women and men should be trained in basic saving schemes in order to be able to have some income set aside for health issues.
Government should create knowledge awareness programs on the existing reproductive health programs and policies especially to the rural community. This should be done through campaigns on birth control, health talks and sensitization of the masses on the importance of small family sizes, as this will reduce on the extreme poverty at the household and government levels.
Areas for Further Research
Since the study could not cover all areas in relation to the access and utilization of CU, the following are the recommended areas for further research:
Research can be carried out to find out how Government is trying to respond to the accessibility and utilization of reproductive health technologies among rural women (married and unmarried). It could look at policies in place that are trying to ensure that women access reproductive health services. Evaluation research could also be carried out on the consequences of cultural and religious beliefs on rural women in access to reproductive health and especially contraceptive use.
23840
References
- Glinski AM, Sexton M, Petroni S (2014) Adolescents and family planning: what the evidence shows. International Center for Research on Women.
- Sileo KM (2014) Determinants of family planning service uptake and use of contraceptives among postpartum women in rural Uganda. pp: 602-610.
- Lowe SMP, Moore S (2014) Social networks and female reproductive choices in the developing world: A systematized review. Reprod Health 11: 85.
- Keele JJ, Forste R, Flake DF (2005) Hearing native voices: contraceptive use in Matemwe Village, East Africa. Afr J Reprod Health 9: 32-41.
- Gipson JD, Hindin MJ (2013) Intergenerational relationships between women’s fertility, aspirations for their children’s education and school completion in the Philippines. J Biosoc Sci 47: 825-844.
- Uganda Bureau of Statistics (UBOS) and ICF International Inc: Uganda Demographic and Health Survey 2016, Kampala, Uganda and Calverton, Maryland: UBOS and ICF International Inc, 2012.
- Esabella Jobu Micheal (2012) Use of contraceptive methods among women in stable marital relations attending health facilities in Kahama district, Shnyanga region, Tanzania. Master of Public Health Dissertation.
- Chabikuli NO, Awi DD, Chukwujekwu O, Abubakar Z, Gwarzo U, et al. (2011) The use of routine monitoring and evaluation systems to assess a referral model of family planning and HIV service integration in Nigeria. AIDS 23: S97-S103.
- World Health Organization (2004) Maternal mortality in 2000: estimates developed by WHO, UNICEF and UNFPA. Geneva: World Health Organization.
- Elizabeth Leahy, Esther Akitobi (2009) A case study of reproductive health supplies in uganda; Population Action International.
- Nketiah-Amponsah E, Arthur E, Aaron A (2012) Correlates of contraceptive use among ghanaian women of reproductive age (15-49 years). Afr J Reprod Health 16: 155-170.
- Asiimwe JB, Ndugga P, Mushomi J (2013) Socio-demographic factors associated with contraceptive use among young women in comparison with older women in Uganda. DHS Working Papers No. 95. Calverton, Maryland, USA: ICF International.
- Aremu O (2013) The Influence of socio-economic status on women’s preferences for modern contraceptive providers in Nigeria: a multilevel choice modeling. Patient Prefer Adherence 7: 1213-1220.
- Graffy J, Goodhart C, Sennett K, Kamusiime G, Tukamushaba H (2012) Young people’s perspectives on the adoption of preventive measures for HIV/AIDS, malaria and family planning in South-West Uganda: focus group study. BMC Public Health 12: 1022.
- Moser C (1993) Gender planning and development, theory, practice and training, london and New York: Routledge Press.
- Elson D (1999) Labor markets as gendered institutions: equality, efficiency and empowerment issues. World Development 27: 611-627.
- Sen G, Grown C (1987 Development, crises and alternative visions: third world women’s perspectives. New York: Monthly review press.
- Newman L (2003) Social research methods: qualitative and quantitative approaches. sage publications, USA.
- Nalwadda G, Mirembe F, Byamugisha J, Faxeli E (2010) Persistent high fertility in uganda: young people recount obstacles and enabling factors to use of contraceptives. BMC Public health 10: 530.
- Wright D, Plummer ML, Mshana G, Wamoyi J, Shigogo ZS, et al. (2006) Contradictory sexual norms and expectations for young people in rural northern Tanzania. Soc Sci Med 62: 987-997.
- Qiang D, Xiaoyun Li, Hongping Y, Keyun Z (2008) Gender inequality in rural education and poverty; Chinese Sociol Anthropol 40: 64-78.
- Mosher WD, Martinez GM, Chandra A, Abma JC, Willson SJ (2004) Use of contraception and use of family planning services in the United States: 1982-2002. Adv Data 10: 1-36.
- Kalule-Sabiti I, Amoateng AY, Ngake M (2014) The effect of socio-demographic factors on the utilization of maternal health care services in Uganda. Afr Popul Studies, pp: 28-32.
- Laurie D, Alex E (2010) Decision-making patterns and contraceptive use: evidence from uganda. Popul Res Policy Rev 29: 423-439.
- Mathole T, Lindmark G, Majokoro F, Ahlberg BM (2004) A qualitative study of women’s perceptive of antenatal care in a rural area of zimbabwe. Midwifery 20: 122-132.
- Adesegun OF, Kayode TL (2003) Federal ministry of health. National study on essential obstetric care facilities in Nigeria. Abuja: Federal Ministry of Health. pp: 20-23.
- Langer A, Meleis A, Knaul FM, Atun R, Aran M, et al. (2015) Women and health: the key for sustainable development. Lacent 386: 1165-1210.
- Balal A, Nelson E (2009) Addressing gaps in family planning access. Marie Stopes International (MSI). London.
- Simkhada B, Teijlingen ER, Porter M, Simkhada P (2007) Factors affecting the utilization of antenatal care in developing countries: systematic review of the literature. J Adv Nurs 61: 244-260.
- Okiezie CA, Ogbe AO, Okezie CR (2010) Socio-Economic Determinants of Contraceptive Use among Rural Women in Ikwuano Local Government Area of Abia State, Nigeria. Int NGO J 5: 74-77.
- Collins CMA (1999) Reproductive technologies for women with physical disabilities. Sex Disabil 17: 299-307.
- Katende C, Gupta N, Bessinger R (2003) Facility-Level Reproductive Health Interventions and Contraceptive Use in Uganda. Guttmacher Institute 29: 130-137.
- Clerand J, Bernstein S, Ezeh A (2006) Family planning the unfinished agenda. Lancet 368: 1810-1827.
- Cohen B (2000) Family planning programs, socio-economic characteristics, and contraceptive use in Malawi. World Dev 28: 843-860.
- Darroch JE, Singh S, Nadeau J (2008) In contraception; an investment in lives, health and development. New York, Guttmacher Institute and UNFPA pp: 1-4.
- Bbaale E, Mpuga P (2011) Female education, contraceptive use, and fertility: evidence from uganda. J Sustain Dev 6: 20-47.
- Elphis C (1991) Family planning and reproductive decisions, J Reprod Infant Psychol 1: 217-226.
- Foreit JR, Frejka T (1998) Family planning operations research: A book of readings, New York: The Population Council.
- Ghana Statistical Service (GSS), Ghana Health Service (GHS) and ICF Macro (2009). Ghana Demographic and Health Survey 2008. Accra, Ghana: GSS, GHS and ICF Macro.
- Grown CG, Gupta R, Khan Z (2003) Promises to keep: achieving gender equality and the empowerment of women. Background paper for the UN millennium project task force on education and gender equality, ICRW (International Center for Research on Women), Washington, D.C.
- https://blog.dsw.org/2015/03/empowerment-of-women-and-girls-is-progress-for-all-three-decades-of-gains-for-ugandan-women-and-girls/#more-2264
- https://www.chinadaily.com.cn/english/doc/2005-01/18/content_410003.htm
- Wang C (2012) Trends in contraceptive use and determinants of choice in China 1980-2010. Contraception 85: 570-579.
- Edmeades J, Hayes R, Gaynair G (2014) Improving the lives of married adolescent girls in amhara, Ethiopia. ICRW pp: 1-12.
- https://www.census.gov/content/dam/Census/library/workingpapers/1994/demo/sp73.pdf
- https://gc21.giz.de/ibt/var/app/wp385P/2371/index.php/events/uganda-empowerment-of-women-and-girls-is-progress-for-all-three-decades-of-gains-for-ugandan-women-and-girls/
- Tian L, Li J, Zhang K, Guest P (2007) Women’s status, institutional barriers and reproductive healthcare: a case study in yunnan, china, health policy 84: 284-297.
- Dynes M, Stephenson R, Rubardt M, Bartel D (2012) The Influence of perceptions of community norms on current contraceptive use among men and women in Ethiopia and Kenya. Health Place 8: 766-773.
- Ministry of Health (MOH) (2009) Annual Health Sector Report 2008/2009, Kampala Uganda.
- Ministry of Health (2000) Health sector strategic plan 2000/2001-2004/2005 Kampala Uganda.
- Shapiro D, Tambase BO (1994) The impact of women's employment and education on contraceptive use and abortion in Kinshasa, Zaire. Stud Fam Plann 25: 96-110.
- Babalola S, Fatusi A (2009) Determinants of use of maternal health services in Nigeria-looking beyond individual and household factors. BMC Pregnancy and Childbirth 9: 43.
- Uganda Bureau of Statistics (2016) Uganda Demographic and Health Survey, 2016; Preliminary Reports, Kampala, Uganda.
- UNDP (2007) Millennium Development Goals: Uganda’s Progress Report 2007. Kampala, United Nations Development Program.
- United Nations Department of Economic and Social Affairs, Population Division; World Contraceptive Use Report, 2014.
- USAID/Africa Bureau (2012) Three successful Sub-saharan Africa family planning programs; lessons for meeting the millennium development goals.
- WHO (2010) World Health Statistics 2010, World Health Organization, Geneva.
- Lakew Y, Reda AA, Tamene H, Benedict S, Deribe K (2013) Geographical variation and factors influencing modern contraceptive use among married women in Ethiopia: Evidence from a National Population Based Survey. Reprod Health 10: 52.

