Keywords
Exclusive breastfeeding; Health education; Family support; Health professional support
Abbreviations
EBF: Exclusive Breastfeeding; PHC: Primary Health Center; HP: Health Provider
Background
Improving infant and young child feeding are key points to prevent morbidity and mortality among these children. Exclusive breastfeeding (EBF) and continued breastfeeding with complementary feeding are the major factors in child survival, growth, and development [1]. The latest findings of a systematic review suggested that EBF with no other foods or liquids for 6 months has several advantages over EBF for 3 to 4 months, and no growth deficits have been demonstrated among infants either in developed or developing countries who are exclusively breastfed for 6 months [2]. EBF has been demonstrated to prevent morbidity and mortality from gastrointestinal infection in developing countries [3]. The World Health Organization (WHO) recommends that infants should be exclusively breastfed until the age of 6 months to achieve optimum growth, development and health [2]. However, despite the well-recognized importance of EBF, the practice is not widespread in developing countries. A trend analysis of data from 66 developing countries showed an increase of only 5% from 33% in 1995 to 39% in 2010 [4].
The ideal nourishment for the first six months of life is breast milk. It provides all the nutrients, minerals and vitamins that an infant requires [5]. Moreover, breast milk helps against multiple diseases, such as gastrointestinal and acute respiratory infections [6-8], thus, reduces infant mortality and helps faster recovery during illness [8]. Breastfeeding has also been reported to stimulate sensory and cognitive development [9,10]. Optimal breastfeeding is expected to prevent 1.4 million deaths among children under five, in developing countries annually [11].
In Indonesia, the national Demographic and Health Survey indicated an increase in the prevalence of EBF, from 37% in 2007 to 42% in 2012 [12,13]. Another national survey reported an EBF prevalence of 34% in 2013 [14]. Although progress has been made in Indonesia, as well as in other developing countries, more than half of the infants did not receive EBF as recommended. As exclusive breastfeeding is a major factor in child survival, its success would affect neonatal death rate.Despite neonatal death rates in Indonesia has been greatly reduced (32 death per 1000 in 1991 to 19 death per 1000 in 2012), the disparity of death rates among regions was still remarkable, with the lowest was 13 in South Sulawesi and the highest was 35 in West Papua province [13,15]. Therefore, strong efforts are needed to improve the prevalence of exclusive breastfeeding. Health education and peer support interventions have been reported to improve the prevalence of breastfeeding.
In the current study, we aimed to report the prevalence of EBF in different regions and to examine whether health education on EBF and support from family/peers and health professionals increase the likelihood that a mother will exclusively breastfeed her infant until the age of 6 months. Findings of this study would have an important contribution to the development of strategies to promote EBF. In order to fulfil our study aims, we reviewed theses and dissertations of students from the Faculty of Public Health, University of Indonesia (FPH UI).
Methods
Search strategy
We reviewed several studies that had been conducted to investigate the influence of breastfeeding promotion and education through health personnel as well as through media, and also examine the effect of family support on the practice of EBF. We used the WHO’s recent definition of EBF, which is to give no other meal except breast milk to newborn until the age of 6 months [2]. We included studies on EBF between 2003 and 2014 because the definition of EBF changed in 2002. Prior to 2002, the period of EBF was until infants reached the age of 4 months. The included studies originated from the Faculty of Public Health and included bachelor's and master's theses, as well as doctoral dissertations. All documents were archived in the Faculty of Public Health Library.
We restricted our search to studies that employed crosssectional and cohort design, and also surveys. Case-control studies were not considered eligible in our search due to the nature of the design which prevents us from calculating the prevalence of EBF. We applied “exposed to breastfeed information”, “family support”, and “health provider support” as the exposure terms and “exclusive breastfeeding” as the outcome terms.
In the initial search (keyword search using lib.fkm.ui.ac.id, a portal of FPH UI online library), we identified 264 studies. The titles and abstracts of these studies were reviewed by three authors independently. The studies were selected for further review if they addressed the followings: 1) exposure to breastfeeding information, education or promotion by health personnel, family, or from media, (2) family and peer support for EBF, and (3) health personnel support for breastfeeding with the practice of EBF. Any disagreement between the three authors was discussed with the lead author to reach consensus. We excluded any qualitative studies, duplication of data (studies using the same data for other objectives, but still related to breastfeeding), and studies that did not address our research questions. In addition, we also select studies which meet our standard, i.e. study design and analysis in accordance with our study aims, study participants were mother of infants aged 6-12 months, and sample size minimum of 80.
This step resulted in 49 studies that potentially fit our selection criteria. Authors then reviewed the full text of those 49 studies, and confirmed that 22 studies meet our selection criteria. The remaining 27 studies were excluded due to various reasons that include the use of different EBF definition, exposure or outcome of the studies did not meet our research questions, potential information bias due to ambiguous questions that could lead to misclassification of exposure status, and inadequate sample size. From the eligible 22 studies, most of them (20 out of 22) were bachelor's theses, and only 2 were master's theses; no eligible studies were found from doctoral dissertations (Figure 1).
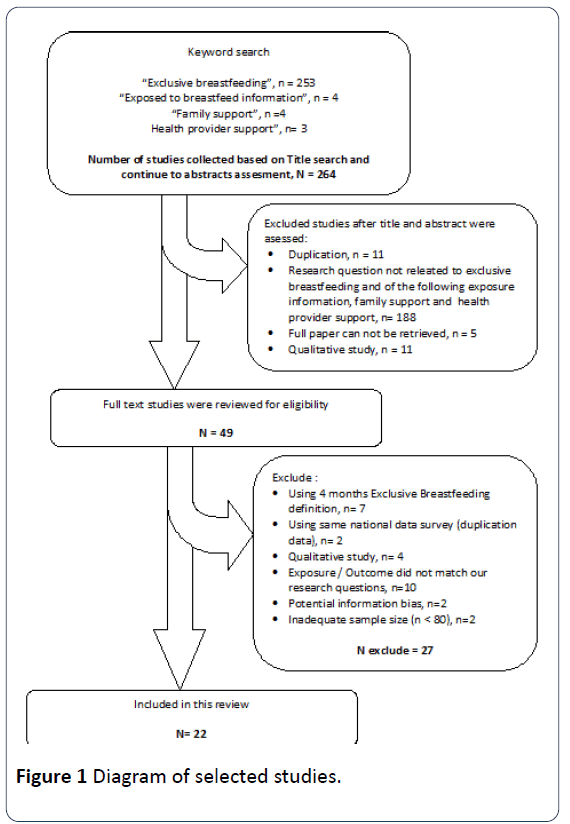
Figure 1: Diagram of selected studies.
Full text of each selected studies was retrieved, and the consistency between the objectives, method and study result in each study were reviewed by three authors. To solved any disagreement among authors, the first author assessed the full text and decided whether to include or exclude the study. Included studies then extracted to inclusion form which consist of study objective, method of collecting data, sample size, and study result.
Data analysis
Descriptive information was presented as proportions. We measured the correlation between the percentage of EBF and exposure of breastfeeding promotion, education, and support based on the correlation coefficient. Linear regression was used to analyze the association of exposed to EBF information, family support, health support and the prevalence of EBF. The associations between mothers’ exposure to EBF information and/or support for EBF and EBF practice were presented as the ORs and 95% CI which were obtained from the original studies.
Results
As can be seen in the map (Figure 2), most of the studies were conducted in Java Island, the most populated area in Indonesia. Some studies were carried out in Sumatra and Sulawesi, which are two other large islands in the country. Thirteen studies were conducted in rural areas, and nine were in urban areas.
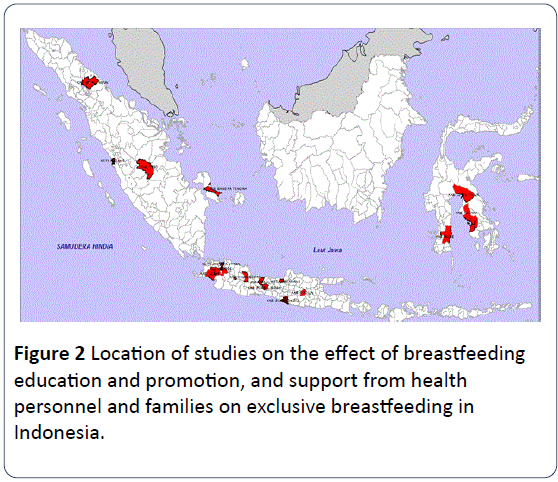
Figure 2: Location of studies on the effect of breastfeeding education and promotion, and support from health personnel and families on exclusive breastfeeding in Indonesia.
Characteristics of the studies included in this review
Table 1 summarizes the characteristics and main results of the 22 eligible studies conducted between 2004 and 2014 by students of FPH UI that examined the association between EBF practice and exposure to breastfeeding information, education or promotion by health personnel, family or from media, and also family and/or health personnel support. Nine studies were done in urban areas, of which, five were carried out in Jakarta Metropolitan areas, the capitol of Indonesia. Three other studies were done on the outskirts of Jakarta, including in the surrounding areas of the University of Indonesia. Seven studies (31.8% of the total studies included) were done outside of Java Island, of which five studies were done in rural areas.
Most of the reviewed studies examined support for EBF from health provider(s), as well as from the families. Exposures to EBF information (from media, family and peers, as well as direct health education) were studied only in 4 studies that were done in rural areas and three studies in urban areas. Most of the studies, both in rural and urban areas, enrolled about 100 to 200 respondents. Only two rural studies and two urban studies included fewer than 100 subjects. By and large, the number of participants in rural studies was comparable to those who participated in urban studies. All studies included in this review employed cross-sectional design.
| No |
Authors and years |
Study locations |
Study settings |
Sample size |
Subject recruit-ment sites |
Percentages of EBF (%) |
Percentages of the presence of facilitating factors for EBF (%) |
| Exposed to EBF information |
Family support for EBF |
HP support for EBF |
| 1 |
Rubinem [16] |
Banyumanik, Semarang, Central Java |
Rural |
100 |
PHC |
23 |
78 |
42 |
59 |
| 2 |
Nofyanti [17] |
Sumberjayes, Majalengka, West Java |
Rural |
122 |
Community |
34.4 |
47.5 |
47.5 |
87.7 |
| 3 |
Intan Meiniwati [18] |
Kebon Sari, Madiun, East Java |
Rural |
115 |
PHC |
49.6 |
85.2 |
78.3 |
73 |
| 4 |
Sudjaroh [19] |
Kramat, Tegal, Central Java |
Rural |
90 |
PHC |
7.8 |
- |
30 |
40 |
| 5 |
Maryani [20] |
Bojongsari, Purbalingga, Central Java |
Rural |
106 |
PHC |
44.3 |
- |
82.1 |
84 |
| 6 |
Asnani [21] |
Wundulako, Kolaka, Southeast Sulawesi |
Rural |
240 |
PHC |
30.8 |
- |
68.3 |
85 |
| 7 |
Muliati Kendek [22] |
Tomoni, Luwu Timur, South Sulawesi |
Rural |
127 |
PHC |
23.6 |
- |
74 |
80.2 |
| 8 |
Elizabeth Nangoy [23] |
Suwawa, Bone, South Sulawesi |
Rural |
100 |
PHC |
23 |
85 |
58 |
64 |
| 9 |
Hajijah Septia Utami [24] |
Koba, Bangka Tengah, Bangka Belitung |
Rural |
105 |
Community |
25.7 |
- |
54.3 |
70.5 |
| 10 |
Yudi Iskandar [25] |
Rimbo Ilir, Tebo, Jambi |
Rural |
144 |
Community |
13.9 |
- |
68.7 |
57.6 |
| 11 |
Christina Legawati Huka [26] |
Cijeruk, Bogor, West Java |
Rural |
210 |
Community |
22.9 |
- |
52.4 |
71.9 |
| 12 |
Ucu Yoanah [27] |
Cipanas, Lebak, West Java |
Rural |
92 |
PHC |
43.5 |
- |
88 |
- |
| 13 |
Tri Agustina [28] |
Wonosari, Gunung Kidul, Central Java |
Rural |
203 |
PHC |
53.2 |
- |
55.7 |
71.2 |
| 14 |
Lutfi Prisma Nurini [29] |
Cilincing, North Jakarta |
Urban |
200 |
PHC |
47.5 |
- |
58 |
62 |
| 15 |
Wiwit Faisal [30] |
Pandang, Padang, West Sumatra |
Urban |
174 |
Community |
29.3 |
- |
59.8 |
58.6 |
| 16 |
Yeye Fahrina Inayatillah [31] |
Astana Anyar, Bandung, West Java |
Urban |
103 |
PHC |
24.3 |
- |
61.2 |
64.1 |
| 17 |
Nur Chowiyah [32] |
Kramat Jati, East Jakarta |
Urban |
87 |
PHC |
37.9 |
- |
43.7 |
56.3 |
| 18 |
Ida [33] |
Beji, Depok, West Java |
Urban |
172 |
Community |
25.6 |
51.2 |
63.4 |
45.9 |
| 19 |
Mery Ramadani [34] |
Padang Utara, Kota Padang, West Sumatra |
Urban |
186 |
Community |
86.5 |
- |
57 |
51.1 |
| 20 |
Nia Afriana [35] |
Tanah Abang, Central Jakarta |
Urban |
218 |
Workplace |
28 |
81.7 |
76.6 |
48.6 |
| 21 |
Anna Andreani Aksa. [36] |
Kebayoran Lama, South Jakarta |
Urban |
120 |
PHC |
63.3 |
- |
84.2 |
- |
| 22 |
Marly Apandi [37] |
Wanasari, Cibitung, Bekasi |
Urban |
210 |
Community |
15.2 |
77.6 |
50 |
48.1 |
Table 1: Characteristics of the 24 studies included for review on the effect breastfeeding education and promotion, and support from health personnel and families on exclusive breastfeeding practice.
The studies included in this review had different sites for subject recruitment. Studies carried out in rural areas mostly recruited eligible subjects among mothers who visited the Primary Health Care (PHC) for any reasons (9 out of 13 studies in rural settings). Only four studies carried out in rural settings recruited subjects from the community where the lists of potential subjects were obtained from posyandu (Pos Pelayanan Terpadu or Integrated service post). Posyandu is a monthly clinic for children and pregnant women at the village level, providing vaccinations and nutritional supplements [15]. On the other hand, studies conducted in urban areas recruited subjects from different sites, such as the PHC, community, and even from the workplace.
Percentage of EBF
The percentages of mothers practicing EBF among all 22 studies ranged widely. The smallest was 7.78%, which was reported by a study done in rural Central Java at a primary health center [16-19], and the highest was 63.3%, which was reported by a study done in urban West Sumatra [20-34]. Central Java province is considered as one of the most welldeveloped areas in the country, while West Sumatra province is likely to be categorized as medium-high developed area. In general, the percentage of mothers practicing EBF was reported to be higher in urban settings than in rural areas (mean percentage of 30.4% in rural areas vs. 39.7% in urban areas), and higher in studies done at the primary health center than those carried out in the community (mean percentage of 36.3% in primary health center vs 31.7% in the community).
We also differentiated the results by regions, comparing findings from studies conducted in and outside Java Island. The Java Island could be considered as the most populated and developed area in the country, in terms of economic and education development, with a higher number of health facilities/personnel. It is also where the capitol city is located. We found that studies that were done outside of Java Island reported relatively lower rates of mothers practicing EBF, especially those carried out in rural areas. The percentage of EBF in Java Island ranged between 7.78% and 63.3% while outside Java Island the percentage was between 13.9% and 86.5%. In the urban areas, the percentage was 24.3%-63.3% in Java Island, lower than outside Java Island (29.3%-86.5%). In rural areas the percentages of EBF were mostly higher in Java Island (7.8%-53.2%) than outside Java Island (13.9%-30.8%).
Factors that potentially facilitate exclusive breastfeeding practice
Factors that potentially facilitate EBF practice among mothers with infants aged older than six months were: 1) being exposed to EBF information from media, family and peers, as well as from health personnel/providers; 2) receiving support from family; and 3) receiving support from the health provider. The results presented here were based on a review of each of the factors mentioned above.
Mothers being exposed to EBF information: Only seven studies evaluated the effects of mothers being exposed to EBF information from all sources, i.e., media (e.g., newspaper, radio, television, and internet), family and peers, and health personnel/providers. Four of the studies were carried out in the rural area while three studies were in the urban setting.
The percentages of mothers exposed to EBF information ranged from 47.5% to 85.2% (Table 1). The percentages were not far different between rural and urban settings. Correlation between percentages of mothers being exposed to EBF information and percentages of EBF practice in the seven studies indicated that there was no association between the two (coefficient correlation r=0.062, p-value 0.921) (Figure 3). Similarly, the linear regression results indicated that there was no association between mothers' exposure to EBF information and their EBF practice. The R-square of the regression was only 0.004, indicating that having a high percentage of mothers exposed to EBF information in a population could not predict a high percentage of mothers practicing EBF.
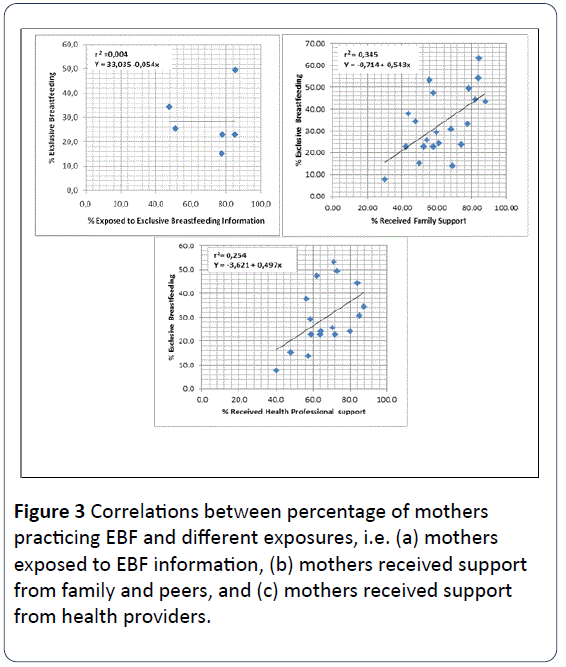
Figure 3: Correlations between percentage of mothers practicing EBF and different exposures, i.e. (a) mothers exposed to EBF information, (b) mothers received support from family and peers, and (c) mothers received support from health providers.
On the other hand, the results seen at the individual study level did not show a similar pattern as the result based on regression analysis above. Findings from individual studies were examined based on the ORs and 95% CI produced by the studies (Figure 4a and Figure 5a). The results showed an increased chance of mothers practicing EBF among those who were exposed to EBF information, but there was one study that had an OR of 0.85, 95% CI: 0.30-2.39 [18]. The largest OR was shown by a study done in rural area in Central Java (N=100) [16] with a very wide confidence interval (OR=8.25, 95% CI: 1.05-65.11). The only study that showed a significant result with somewhat narrow confidence interval was the study done in the rural community setting in West Java (OR=2.44, 95% CI: 1.13-5.25; N=122) [17].
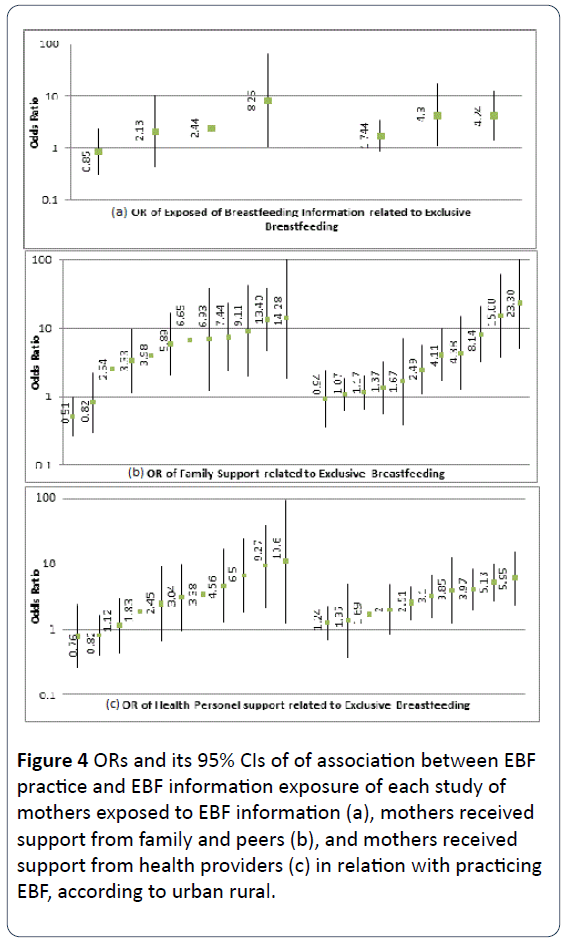
Figure 4: ORs and its 95% CIs of of association between EBF practice and EBF information exposure of each study of mothers exposed to EBF information (a), mothers received support from family and peers (b), and mothers received support from health providers (c) in relation with practicing EBF, according to urban rural.
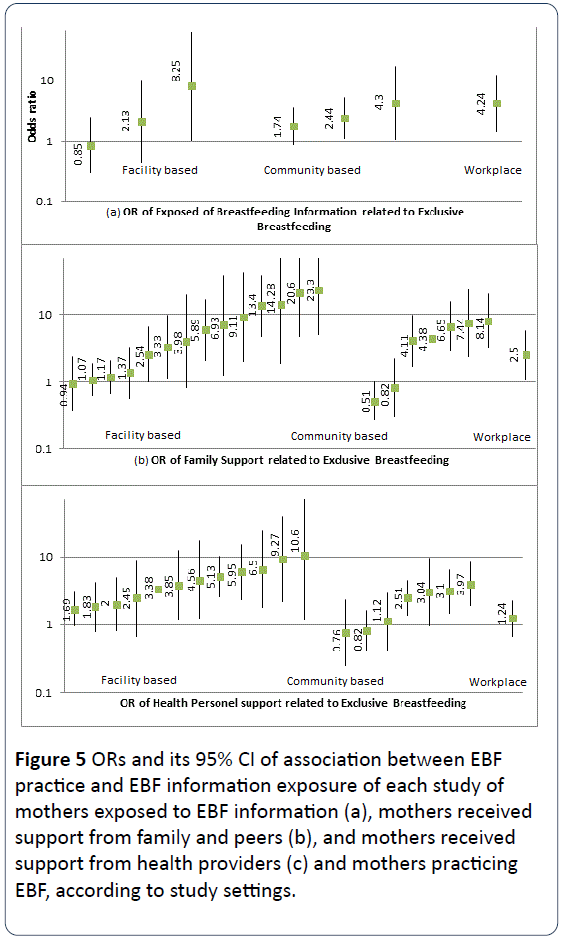
Figure 5: ORs and its 95% CI of association between EBF practice and EBF information exposure of each study of mothers exposed to EBF information (a), mothers received support from family and peers (b), and mothers received support from health providers (c) and mothers practicing EBF, according to study settings.
When stratified by the location where the study subjects were recruited, we found that there was only one study done in a workplace setting. This study demonstrated a significant association (OR=4.24, 95% CI: 1.44-12.48) [35]. Three studies were done in a health facility (primary health center), of which only one showed a significant association between exposure to EBF information and EBF practice [16]. Three other studies were done in community settings, all of which showed a significant association between the exposure to EBF information and EBF practice.
Mothers receiving support from family and peers to practice EBF: All of the 22 studies included in this review evaluated the effect of support from families and peers on mothers’ EBF practice EBF, of which 13 studies were done in rural settings, and nine were in urban areas. The studies included in this review reported that between 30% and 88.04% of mothers received support from families and peers to practice EBF (Table 1). The percentages of mothers receiving family and peer support for EBF reported in studies in the urban setting were not as widely varied compared to those reported in rural studies (30%-88.04% vs. 50%-83.8%, respectively). Correlation between the percentages of mothers receiving family and peer support for EBF and percentages of EBF practice indicated a positive association between the two (r=0.587, p value=0.005) (Figure 3). Regression of the two percentages indicated a positive relationship between mother receiving family and peer support for EBF and EBF practice. The R-square of the regression was 0.345, indicating that having a high percentage of mothers receiving family and peer support for EBF in a population would be followed by a high percentage of mothers practicing EBF.
Most of the studies demonstrated ORs that indicated significant positive associations between the support and the practice of EBF, ranging from 2.54 (95% CI: 0.99-6.48) [18] to 14.28 (95% CI: 1.86-109.57) [21] in studies done in rural settings and from 4.11 (95% CI: 1.71-9.91) [33] to 23.30 (95% CI: 5.04-107.59) [36] in urban settings. There were several studies that showed no effect or non-significant weaker effects, which were mostly indicated by studies carried out in urban sites. These study results revealed that there was a stronger effect of support from family and peers for EBF in rural settings than in urban areas.
The associations mentioned above were also evaluated based on the location where the participants were recruited, i.e., health facilities (primary health center), community, and workplace (Figure 4b). There was only one study done in the workplace, which was not surprisingly located in an urban area. This study showed an increased chance of practicing EBF with the support of family (OR= 2.50, 95% CI: 1.10-5.69). Among the 14 facility-based studies, ten studies showed a significant association between family/peers support exposure and EBF practice [16]. Seven other studies were done in community settings, 5 of which showed significant relationships between thefamily/peers support exposure and EBF practice.
Mothers receiving support from health providers to practice EBF: There were 20 studies evaluated the effect of support from health providers on EBF practice; twelve studies were carried out in rural settings and eight were in urban areas. The percentages of mothers receiving support from the health provider to practice EBF reported by the 20 studies ranged from 48.1% to 87.7%. Mothers in rural areas were reported to receive higher support from health providers for EBF compared to those reported in urban areas (59.0% to 87.7% versus 48.1% to 64.1%, respectively) (Table 1). Percentages of mothers receiving support from health providers for EBF showed a positive correlation with EBF practice (r=0.504, p value=0.028). The R-square of the regression was 0.254, indicating that having a high percentage of mothers receiving support from health providers for EBF in a population would be followed by a high percentage of mothers practicing EBF.
Figure 4c shows the associations between health provider support and EBF practice according to rural versus urban settings. The effects of support from health providers for EBF practice were more substantial in rural areas compared to those in urban settings. Six out of 11 studies carried out in rural settings showed that support from health providers is associated with increased likelihood of mothers to practice EBF. The associations were of a high magnitude, although one of the Ors showed a borderline significance: ranging from 3.38 (95% CI: 1.05-10.88) [23] to 10.6 (95% CI: 1.22-92.27) [19]. The likelihood of mothers practicing EBF related to health provider support reported from studies carried out in urban settings were found to be between 2.51 (95% CI: 1.39-4.54) [34] to 5.95 (95% CI: 2.33-15.18) [36].
The effects of health provider support for EBF were more extensive in studies that recruited subjects from health facilities compared to the community. There was only one study that recruited samples from the workplace, and such effect was not found. The range of significant effects in studies done in health facilities was reported from 1.69 (95% CI: 0.95-3.02) [29] in urban areas to 10.6 (95% CI: 1.22-92.27) in rural areas [19]. The significant effects reported from studies done in the community setting were mostly of lower magnitudes, ranging from 2.51 (95% CI: 1.39-4.54) [34] to 3.97 (95% CI: 1.90-8.33) [33]. By and large, majority of the included studies were found to show significant effects (Figure 5b and c).
Discussion
This current study evaluated studies of students in the FPH UI on EBF between 2003 and 2014. Our search strategy followed that of a systematic review. We did not calculate the pooled estimate because of the sources of our study were restricted to bachelor's and master's theses that were listed in the library (no doctoral dissertation that fulfilled our study aim was found). Therefore, the results could still be biased from the true value because bachelor's and master's theses done at the University of Indonesia might not be representative of results from the other theses or research done in other university or area. Although the source was the library database, our review included studies from several different parts of Indonesia, such as Metropolitan Jakarta, West Java, Central Java, East Java, Sumatra, and Sulawesi.
The prevalence of EBF in the studies included in this review was found to be higher in urban than in rural settings (mean prevalence of 39.7% and 30.4%, respectively). These figures are not different from the previously reported prevalence, nationally [12-14] or internationally [11]. Our investigation found that among the strategies to improve the prevalence of EBF (i.e., being exposed to EBF information from media, family, peers and health professionals, or received support from family and peers, or received support from health providers), being exposed to EBF information from a variety sources seems to have the least effect on EBF practice although the least effects were still of large magnitudes. Exposure to EBF information seems to have a positive effect among mothers recruited in the workplace, despite the fact that it is only based on one study done in Central Jakarta (in a government institution) [35]. The prevalence of EBF in the study conducted in a workplace was not high (28%); however, being exposed to EBF information was associated with a four-fold increase in the likelihood of practicing EBF. A study in Southeast Ethiopia found that employed mothers were less likely to practice EBF [37-39]. To improve this situation, providing systematic information about EBF, coupled with creating an enabling, breastfeeding-friendly working environment for working mothers is recommended. EBF education, in a study in rural Bangladesh, was reported to have no increased likelihood of practicing EBF [40]. Our results showed that exposure to EBF information was also less effective at increasing the likelihood of practicing EBF; however, our library did not have many studies that analyzed the exposure to EBF information.
In our study, a higher effect was observed among mothers who received support for EBF.This indicates the importance of social and emotional support from a partner and other family members on breastfeeding which has also been reported by a study in Bristol, UK [41]. Another study, a literature review done by Shahla et al. in New South Wales found that women who intend to breastfeed for a longer period and are well supported by their family demonstrated positive and prolonged breastfeeding behaviour [42]. Similar results were found among the studies being reviewed in this current analysis, that support from family and peers seems to improve the practice of breastfeeding in almost all of the studies included. However, the effects were more apparent among women living in urban areas as opposed to those in rural settings. It might be that more women in urban settings were working mothers, and thus, the role of family caregiver becomes crucial in breastfeeding the infant with milk that has been expressed by the mother and kept in the refrigerator. However, in rural areas, most women do not work outside the house, and hence, the issue of family member support becomes less critical.
The present study also found a significant effect of health provider’s support on EBF practice. The result was consistent with a systematic review that reported a pooled estimate of the effect of health professional support for EBF (OR=1.14; 95% CI: 1.06-1.22) [43]. In our study, the role of health provider's support on EBF practice was found to be of a lesser scale compared to those of family support, both in urban and rural settings. The effects of health providers’ support on EBF practice in studies that recruited subjects in health facilities is stronger than in community-based studies. Such a role was insignificant among working mothers, however. Unfortunately, this study was not able to directly attribute this finding to particular characteristics of subjects recruited in the facility, compared to subjects recruited in the community or workplace, to explain the different findings by subject recruitment location. However, the stronger findings in facilitybased studies could indicate the potential opportunity for health education and support in health facility setting to obtain a higher effect on EBF practice.
Our review has some limitations which stem mainly from the methodological weaknesses of the included studies. The possibility of a variety of biases including selection (which related to the type of population and sample size) and information bias could not be ruled out. The large confidence intervals found in many of the included studies might be a hint of the chance due to the small sample size that might have occurred in the studies. However, judging from the wide range of EBF prevalence, and the prevalence of the facilitating factors for EBF, the biases that might be present were not systematically in one direction. Thus, if a pooled estimate is being calculated, the likelihood of excessive underestimation or overestimation would be of a lesser magnitude.
The lessons learned from this qualitative review are that all strategies to improve the practice of EBF were effective. However, considerations should be made based on the type of mothers (the target) when carrying out a strategy for intervention to promote EBF. If the target is working mothers, the role of health professional support would be of lesser magnitude. In this group, family and peer (friends) support, as well as adequate EBF information, seems to be more effective, presumably using currently available modes of communication such as Twitter and Facebook. For housewives who might not go to a health facility too often, family, as well as health professional supports, would be the best option for women in urban as well as in rural areas.
Competing interests
The authors declare that they have no competing interests.
Authors’Contributions
A.C.A concepting, write, supervise and finalizethe paper; S.Maemun, W.Sari and Ritanugraini decide the topic, collect the data, and write the draft of paper; S.Choirunisa analyze the data, write, finalize the paper.
Acknowledgement
This paper has been reviewed by Gina Samaan (US CDC for Field of Epidemiology Training Programme Indonesia).
17360
References
- Jones G, Steketee RW, Black RE, Bhutta ZA, Morris SS, et al. (2003) Child survival II: How many child deaths can we prevent this year? Lancet Child Survival Series 362: 65-71.
- Kramer MS, Kakuma R (2009) Optimal duration of exclusive breastfeeding (Review). Cochrane Library. Kramer MS, Kakuma R (WHO) (2011) The optimal duration of exclusive breastfeeding: report of an expert consultation. World Health Organization Geneva, Switzerland.
- Cai X, Wardlaw T, Brown DW (2012) Global trends in exclusive breastfeeding. Int Breastfeed J 7:12.
- Butte NF, Lopez-Alarcon MG, Garza C (2002) Nutrient adequacy of exclusive breastfeeding for the term infant during the first six months of life. World Health Organization, Geneva, Switzerland.
- Beaudry M, Dufour R, Marcoux S (1995) Relation between infant feeding and infections during the first six months of life. J Pediatr 126:191-197.
- Howie P, Forsyth J, Ogston S, Clark A, Florey DVC (1990) Protective effect of breast feeding against infection. Br Med J 300:11-16.
- Kramer MS, Chalmers B, Hodnett ED, Sevkovskaya Z, Dzikovich I, et al.(2001) Promotion of breastfeeding intervention trial (PROBIT): A randomized trial in the Republic of Belarus. JAMA 285: 413-420
- Anderson JW, Johnstone BM, Remley DT(1999) Breast-feeding and cognitive development: a meta-analysis. Am J ClinNutr 70:525-535
- Jedrychowski W, Perera F, Jankowski J, Butscher M, Mroz E, et al.(2012) Effect of exclusive breastfeeding on the development of children’s cognitive function in the krakow prospective birth cohort study. Eur J Pediatr, January 171: 151-158.
- Black RE, Allen LH, Bhutta ZA, Caulfield LE, OnisDM, et al.(2008) Maternal and child undernutrition: Global and regional exposures and health consequences. The Lancet, 371:243-260.
- Statistics Indonesia (BadanPusatStatistik—BPS), Macro International (2008) Indonesia demographic and health survey 2007. Calverton, Maryland, USA: BPS and Macro International
- Statistics Indonesia (BadanPusatStatistik—BPS), National population and family planning board (BKKBN), Kementeriankesehatan (Kemenkes—MOH), ICF International (2013) Indonesia Demographic and Health Survey 2012. Jakarta, Indonesia: BPS, BKKBN, Kemenkes, and ICF International.
- National institute of health research and development, Ministry of health, republic of indonesia(2013) Report on result of national basic health research (Riskesdas). Jakarta: MOH.
- Ministry of Health, Indonesia (2012)Bukupeganganposyandu(Guide book of integrated service post). Jakarta, Indonesia: Ministry of Health.
- Rubinem(2012) Factors associated with exclusive breastfeeding practice in puskesmas (phc) srondol, semarang, Undergraduate Thesis, University of Indonesia, Depok.
- Nofyanti(2012) Factors that influence exclusive breastfeeding in sumberjayasubdistrict, Majalengka, West Java Province, Undergraduate Thesis, University of Indonesia, Depok.
- Meiniwati I (2011) Association between mother’s occupational, other factors and exclusive breastfeeding in Puskesmas (PHC) Kebonsari, Kebonsarisubdistrict, Madiun, East Java Province, Undergraduate Thesis, University of Indonesia, Depok.
- Sudjaroh(2012) Factors associated with exclusive breastfeeding practice in catchment area of work puskesmas(PHC) BangunGalihTegal 2012, Undergraduate Thesis, University of Indonesia, Depok.
- Maryani(2012) Overview of exclusive breastfeeding and the associated factors in work area Puskesmas (PHC), Purbalingga district, Central Java province, Undergraduate Thesis, University of Indonesia, Depok.
- Asnani(2013) Factors associated with exclusive breastfeeding in puskesmas(PHC) Wundulako, Kolaka, Undergraduate Thesis, University of Indonesia, Depok.
- Kendek M (2013) Factors associated with exclusive breastfeeding in puskesmas(PHC) Tomonu, UwuTimur, Undergraduate Thesis, University of Indonesia, Depok.
- Nangoy E (2013) Factors associated with exclusive breastfeeding in puskesmas(PHC) Suwawa, Bone Bolango District, Gorontalo Province, Undergraduate Thesis, University of Indonesia, Depok.
- Utami HS (2012) Factors associated with exclusive breastfeeding practice in puskesmas(PHC) Koba, Bangka Tengah District, Undergraduate Thesis, University of Indonesia, Depok.
- Iskandar Y (2011) Association between mother’s attitude, other factors and exclusive breastfeeding to infants 6-12 months in Puskesmas (PHC) Alai Ilir, Tebo district, Jambi Province, Undergraduate Thesis, University of Indonesia, Depok.
- Huka CL (2010) Factors associated with exclusive breastfeeding practice in puskesmas(PHC) Cijeruk, Bogor, West Java Province. Undergraduate Thesis, University of Indonesia, Depok.
- Yoanah U (2010) Factors associated with exclusive breastfeeding practice in work area of puskesmas(PHC) DTP Cipanas, Lebak, Banten Province, Undergraduate Thesis, University of Indonesia, Depok.
- Agustina T (2011) Determinants of exclusive breastfeeding in puskesmas(PHC) Wonosari, GunungKidul, Yogyakarta Province, Undergraduate Thesis, University of Indonesia, Depok.
- Nurini LP (2009) Factors associated with exclusive breastfeeding practice among multiparae mother in maternal and child health unit in puskesmas(PHC) Cilincing, Undergraduate Thesis, University of Indonesia, Depok.
- Faisal W (2011) Factors associated with exclusive breastfeeding practice in puskesmas(PHC) Padang Pasir, Undergraduate Thesis, University of Indonesia, Depok.
- Inayatillah YF (2010) Factors associated with exclusive breastfeeding practice in work area of puskesmas (PHC) Pagarsih, Bandung, Undergraduate Thesis, University of Indonesia, Depok.
- NurChowiyah(2010) The roles of health provider on exclusive breastfeeding in puskesmas (PHC) KramatJati, Undergraduate Thesis, University of Indonesia, Depok.
- Ida (2011) Factors associated with 6 months exclusive breastfeeding in work area of Puskesmas (PHC) KemiriMuka, Depok, Thesis, University of Indonesia, Depok.
- Ramadani M (2009) Association between partner support and exclusive breastfeeding in work area puskesmas (PHC) Air Tawar, Kota Padang, West Sumatra, Thesis, University of Indonesia, Depok.
- Afriana N (2004) Analysis of exclusive breastfeeding practice among mothers working in government office in Jakarta, Thesis, University of Indonesia, Depok.
- Akse AA (2013) Factors associated with exclusive breastfeeding practice in puskesmas(PHC) Kebayoran Lama, South Jakarta, Undergraduate Thesis, University of Indonesia, Depok.
- Apandi M (2014) Overview of factors associated with exclusive breastfeeding in 30 Posyandu in work area of Puskesmas (PHC) Wanasari, Cibitung, Bekasi, Undergraduate Thesis, University of Indonesia, Depok.
- Dyson L, McCormick FM, Renfrew MJ(2005) Interventions for promoting the initiation of breastfeeding (Review). Cochrane Database of Systematic Reviews 2: CD001688.
- Setegn T, Belachew T, Gerbaba M, Deribe K, Deribew A, et al.(2012) Factors associated with exclusive breastfeeding practices among mothers in Goba district, south east Ethiopia: a cross-sectional study. Int Breastfeed J 7: 17.
- Joshi PC, Angdembe MR, Das SK, Ahmed S, Faruque ASG et al.(2014) Prevalence of exclusive breastfeeding and associated factors among mothers in rural Bangladesh: a cross-sectional study. Int Breastfeed J 9: 7.
- Ingram J, Johnson D, Greenwood (2002) Breastfeeding in bristol: Teaching good positioning, andSupport from fathers and families. Midwifery, 18: 87-101.
- Shahla M, Fahy K,Kable AK (2010) Factors that positively influence breastfeeding duration to 6 months: a literature review. Women Birth. 23: 135-145.
- Imdad A, Yakoob MY, Bhutta ZA(2011) Effect of breastfeeding promotion interventions on breastfeeding rates, with special focus on developing countries. BMC Public Health 11:S24.

