Keywords
Demographic; Cardiovascular; Natural death; Postmortem
Introduction
The World Health Organization (WHO) defined sudden unexpected natural death (SUND) as deaths which occur within 1 to 24 hours after the onset of symptoms [1-3]. This event is not only tragic to the deceased relations and of concern to the coroner but may also have some predictive genetic implications for the surviving relatives [4]. Under the British system, all cases of sudden death which is not seen by a doctor within 14 days preceding death should be autopsied [5]. It is noteworthy that not all SUND has identifiable cause even after extensive investigation [5,6]. Several reports from developed countries indicate that the diseases of cardiovascular system are the most common cause of SUND. For instance, the incidence of sudden cardiac death in the USA, Ireland, China, Japan, UK/Wales and South Africa is 153, 51.2, 41.8, 37, I.8 and 6.4 per 100,000 respectively [7-12]. Chugh et al. [13] reported that the global burden of sudden unexpected natural death accounts for an estimated 4-5 million deaths annually [13]. Despite the dominant involvement of the cardiovascular system, disease of any other organ system can result in SUND. For instance, majority of the sudden unexpected deaths reportedly involved the respiratory, central nervous, gastrointestinal and urogenital systems [14,15].
In Nigeria, there is paucity of reports of SUND. The available reports reflect the major causes of SUND in three of the six geopolitical zones of which the southeast Nigeria is yet to be inclusive [4,16-20]. Similar to the reports from developed countries, with the increasing modernization of lifestyle and dietary habits, cardio-vascular system diseases-particularly complications of hypertension have become the leading cause of sudden unexpected natural death (SUND) in our environment [16].
The aim of this study was to describe the demographic data, the immediate cause of death and associated risk factors in the sudden unexpected natural death cases in Owerri, Imo state, southeast Nigeria.
Methodology
Study design
This is a retrospective postmortem study.
Study area
Owerri is the capital city of Imo State in Nigeria, set in the heart of Igboland [6]. It is also the state's largest city, followed by Orlu and Okigwe as second and third respectively. Owerri consists of three Local Government Areas including Owerri Municipal, Owerri North and Owerri West, it has an estimated population of about 1,401,873 as of 2016 and is approximately 100 square kilometres (40 sq mi) in area. Owerri is bordered by the Otamiri River to the east and the Nworie River to the south [21].
Study population
Owerri consists of three Local Government Areas including Owerri Municipal, Owerri North, and Owerri West. It has an estimated population of about 401,873 as of 2006 [22] and has area of approximately 100 square kilometers (40 sq m). Owerri is bordered by the Otamiri River to the east and the Nworie River to the south [23,24].
Materials and Methods
The duration of this study was from January 2003 to December 2012. The archived case notes, post-mortem registers and reports were retrieved from database of the Medical records and biostatistics as well as the Department of Pathology of Federal Medical Centre (FMC) Owerri respectively. Cases of sudden unexpected deaths investigated through autopsy with complete post-mortem examinations performed by consultant pathologists in the department using laid down protocols were included in the study. However, autopsy reports with inconclusive cause of death, poorly documented findings, cases that stayed on admission beyond 24 hours and those without prerequisite ancillary investigations were excluded from the study. The demographic characteristics of the patients, social and medical histories, immediate cause of death and comorbidities with corresponding histology findings, microbiological, ancillary clinical and postmortem investigations to confirm the diagnoses seen by naked eye inspection were collected. All the anthropometric variables were measured with metric rules and weighing scales. The most important associated risk factor detected in the patients was selected for the study. The data were analyzed with respect to age, sex, associated risk factors, primary disease and immediate cause of death.
Analytical process
The data was analyzed using SPSS version 16.
Ethical considerations
Ethical clearance for this study was obtained from Research ethics committee Federal Medical Centre Owerri. The certificate number is FMC/OW/HREC/138.
Results
In the period under review (January 2003 to December 2012) 486 medico-legal autopsies were performed. The cases that satisfied the inclusion and exclusion criteria of this study were 47 accounting for 9.7% of all post-mortem carried out in the Department of Pathology FMC Owerri within the period. The male to female ratio was 3.3:1 with mean age of 45.2 ± 17.0. The age range was 15 to 80 years. The peak age of incidence was in the 41-50 years age group. 17.6% of the subjects were obese and 28.8% has complicated atherosclerosis of thoracic aorta. The age groups involved were 10-20, 21-30, 31-40, 41-50, 51-60, 61-70, 71-80 which constituted 4.3% (2 cases), 21.3% (10 cases), 17.0% (8 cases), 25.5% (12 cases), 12.8% (6 cases), 10.5% (5 cases), 8.5% (4 cases) respectively. These age group distributions of the SUND in Owerri are shown in the Histogram below.
Sudden death related to hypertensive cardiovascular disease and its complications occurred in twenty-six subjects. This accounted to for 55.4%. The average cardiac weight and left ventricular wall thickness were 519.3 ± 80.7 with a range of 375-650 g and 2.5 ± 0.4 cm with a range of 2.0 to 3.0 cm respectively. Males constituted 73.33% (19) of cases giving a gender disparity of 2.75:1 and involved people from 22 to 80 years. The mean age for both sexes was 51.0 ± 15.4. Males had a lower mean age of 48.65 years compared to 56.75 years for females. 17.02% (8 cases), 27.66% (13 cases) of the subjects were obese and had complicated atherosclerosis of thoracic aorta respectively. Other associated risk factors included dietary factors 29% (14 cases), alcohol use or misuse 19.15% (9 cases), Cigarette smoking 17.02% (8 cases), diabetes mellitus 12.76% (6 cases), family history of sudden death 10.64% (5 cases), congenital anomalies 4.25% (2 cases) and those without identifiable risk factors 6.38% (3 cases) respectively. These risk factors may be single or in multiples in a single patient. These risk factors are illustrated in the pie chart below.
Three patients died of gastrointestinal tract-related diseases. These patients were aged 23, 48 and 52 years respectively. The youngest died of perforated gastric ulcer with massive haemoperitoneum, peritonitis and haemorrhagic shock. The remaining two died of ruptured esophageal varices consequent upon chronic liver disease with liver cirrhosis and portal hypertension. Other anatomic pathologic finding was haemorrhagic shock evident on the marked corticomedullary differentiation of the kidneys. One of the patients diagnosed with chronic liver disease also had lobar pneumonia as comorbidity.
The central nervous system recorded ten cases. Two were cases of acute bacterial meningitis in a 15 and 45 year old male patients. The male to female ratio was 2.3:1 with mean age of 38.4 ± 10.7 years and age range of 15 to 47 years. The peak age of incidence was 41-50 years with a modal age of 45 years. These patients had prominent leptomeningeal vascular congestion, purulent exudates on the cerebral hemispheres and base of the brain respectively and raised intracranial pressure with tonsillar herniation into the foramen magnum. The microbiology culture yielded Klebsiella spp and Streptococcus pyogenes. The second anatomic pathologic findings in the CNS were intracranial haemorrhage. The subarachnoid haemorrhage had male preponderance with a male to female ratio of 2.5:1. Most (87.5%) of the subjects who were victims of intracranial haemorrhage were obese and had complications of systemic hypertension. Moreover, there is a berry aneurysm circle of Willis in two cases.
Two cases of respiratory diseases were observed. One patient had chronic lung disease (Bronchial asthma) with pulmonary fibrosis, adhesion of the visceral to the parietal pleura with plugging of the bronchioles by thick, tenacious mucus and right atrial and tricuspid valve dialatation. A second case was acute alcoholic intoxication with aspiration of gastric content into the lungs. This patient also had marked cerebral edema (Table 1).
Table 1 Classification of causes of sudden unexpected natural death and the gender distribution.
| s/n |
Organ system |
Cause of death |
M |
F |
Freq |
% |
Sub total |
| 1 |
CVS* |
Hypertensive heart disease |
11 |
3 |
14 |
29.8 |
55.40% |
| Acute left ventricular failure |
5 |
3 |
8 |
17 |
| Congestive heart failure |
1 |
1 |
2 |
4.3 |
| Hypertrophic cardiomyopathy |
1 |
1 |
2 |
4.3 |
| 2 |
GIT* |
Chronic liver disease with ruptured esophageal varices |
2 |
1 |
3 |
6.4 |
8.50% |
| Peptic ulcer disease with perforation |
1 |
0 |
1 |
2.1 |
| 3 |
CNS* |
Acute bacterial menigitis |
2 |
0 |
2 |
4.3 |
21.30% |
| Intracranial haemorrhage |
5 |
3 |
8 |
17 |
| 4 |
RESP* |
Chronic lung disease |
1 |
0 |
1 |
2.1 |
4.20% |
| Aspiration of gastric content |
1 |
0 |
1 |
2.1 |
| 5 |
Vascular |
Complicated atherosclerosis with aortic dissection |
1 |
0 |
1 |
2.1 |
4.20% |
| Obesity with pulmonary embolism |
0 |
1 |
1 |
2.1 |
| 6 |
Undetermined |
|
3 |
0 |
3 |
6.4 |
6.40% |
| Total |
|
|
34 |
13 |
47 |
100 |
100 |
*CVS: Cardiovascular System, GIT: Gastrointestinal System, CNS: Central Nervous System, RESP: Respiratory System, M: Male, F: Female
Vascular diseases accounted for 4.2% (2 cases) of the cases involving two individuals who had complicated atherosclerosis with aortic dissection and cardiac tamponade. The second case had morbid obesity with pulmonary embolism. The cause of death in 6.3% of the cases (3) was not concluded after a comprehensive postmortem examination. All were between the age of 20 and 30 years with mean age of 25.67 years (Figures 1 and 2).
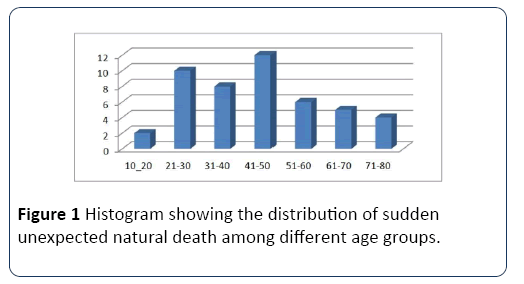
Figure 1: Histogram showing the distribution of sudden unexpected natural death among different age groups.

Figure 2: A pie chart showing the risk factors of sudden natural death in Owerri, Imo State.
Discussion
Sudden unexpected natural deaths (SUND) are public health problems accounting for 15-20% of all death worldwide [25]. In this study, SUND constituted 9.7% of all medico-legal autopsies in Owerri within the period under review. The disease of the cardiovascular system (CVS), central nervous system (CNS) and the gastrointestinal system were the leading primary causes of death and constituted 55.4%, 21.3% and 8.5% respectively. Other organ systems involved were the vascular and respiratory tract diseases which together contributed 8.4%. There was significant gender disparity in the incidence of SUND in our study with male to female ratio of 3.3:1. The mean age was 45.2 ± 17.0 years with peak age of incidence in the 41-50 years age group. The commonest risk factor was dietary factors which constituted 29%, followed by alcohol use or misuse (19.15%), cigarette smoking (17.02%), diabetes mellitus (12.76%) and family history of sudden unexpected death (10.64%).
The contribution of SUND (9.7%) to medicolegal autopsies in Owerri appeared relatively small compared to reports from other parts of Nigeria. This observation is similar to those reported from Port-Harcourt, Ile-Ife and Oshogbo where SUND constituted 10.3%, 13.4% and 4% respectively.4,16,17 However, in Benin City, Makurdi and South Africa SUND constituted 30.3%, 46.4% and 79.0% respectively of all medicolegal autopsies [14,16,20].
The gender disparity in this study is similar to those reported from Makurdi, Ireland, Turkey, Spain and India [8,20,25-28]. Other reports from Nigeria, USA, China, Turkey and Kingdom of Saudi Arabia indicated that the gender disparity were less marked and ranged from 1.7:1 to 2.2:1.4 [16,17,19,29-31]. However, reports from southwest Nigeria were akin to those of India, Iran and Jamaica with a wider male to female ratio ranging from 5:1 to 10:1 [17,19,32,33], Hayashi et al. [24] reported that these sex differences in sudden death may not easily be explained. However, it may be the result of certain demographic and physiologic differences in the gender that confers relative protection to females. For instance, women especially at younger ages, appear to have higher rate of successful cardiopulmonary resuscitation and survival from arrhythmias, possibly due to favorable effects of smaller body size and/or estrogen on success of defibrillation and/or post-resuscitation hemodynamics. Secondly, in cardiac arrest survivors and sudden cardiac death autopsy series, coronary heart disease was found in 45–50% of women compared to 80–90% of men. Moreover, cardiac events occur in women at older age (postmenopausal age) compared to men [24]. In USA, Zheng et al. [28] observed that the gender differences disappeared after the age of eightyfive.
The peak age of incidence in our study was in the 41-50 years age group, with a mean age of 45.2 ± 17 and a range of 15-80 years. This agreed with previous studies from most parts of Nigeria, Turkey and South Africa [4,13,16,17,25]. However, Ngbea et al. [20] reported that the peak age of incidence of SUND in Markurdi, north-central Nigeria was in the 50-60 year age groups. This report agreed with studies from Ireland, USA, India and china where there is a steady rise in the age at which most victims had sudden death [7-9,17,34]. China Society of Pacing and Electrophysiology (CSPE) reported an average age at sudden death to be 58.5 ± 13.8 years compared to 67.2 ± 12.1 years reported by the USA Obesity, Metabolism and Nutrition Institute (US OMNI). The differences reflect the impact of genetics, race and social environment in the development of cardiac diseases and subsequent sudden death [9]. Carnethon et al. [35] reported that the cause of the earlier age in the black population is due to the prevalence of the risk factors for sudden cardiac death such as hypertension, heart failure and peripheral vascular diseases. They also noted that despite the tailored pharmacotherapies for the African-Americans the management of cardiac diseases is less effective. This disparity is multifactorial and stems from individual to the social environment especially the poor health seeking behaviors among African-Americans [35]. However; Anderson et al. [36] observed that the major risk factor for American-Indians is alcohol abuse.
The commonest cause of death in our study was complications of hypertension which included hypertensive heart disease, congestive cardiac failure, and acute left ventricular failure. Hypertensive cardiovascular disease accounted for (26 cases) 55.4%. Similar observations were made in Benin City, Oshogbo, India respectively [14,19,37]. Studies in other parts of Nigeria showed that SUND related to hypertensive cardiovascular diseases constituted 28.3%, 39.3%, 87.5% in Ile- Ife, Benin City, and Port Harcourt respectively [4,16,17]. Moreover, 72.5% and 93.4% of cardiovascular-related SUND were reported from Iran and UK respectively [33,38].
The risk factors identified in this study had more direct impact on the cardiovascular system-related sudden unexpected deaths. They were dietary factors, alcohol use, cigarette smoking, diabetes mellitus and congenital malformations. In a couple of cases (6.4%), no real risk factor was identified. Dietary factor was the commonest risk factor as the clinical history of most victims did not reflect any pattern of healthy eating habits. Traditional diets in Sub-Saharan Africa which are low in fat and high in unrefined carbohydrates protect against cardiovascular diseases. However, there is huge nutritional transition in composition and structure of diet resulting in diet with high fat content - particularly saturated fat, low carbohydrates, fruit, and vegetables, as well as high salt intake which may lead to the emergence of cardiovascular risks [1]. There is an increase in the patronization or dependence on the fast food centres for burger, meat pies and polished white rice in Nigeria today. These western-type diets have less nutritional value than the whole grain and may have less effect on the lowering of blood pressures in the hypertensive patients than the brown rice and traditional African foods. Moreover, there is no much knowledge of the guide line to healthy eating in Nigeria and its attendant financial implication [39]. Moreover, cardiovascular causes of SUND are amenable to certain micronutrients used in the fortification of foods. For instance, Nishimura et al. and Fayed et al. [40,41] reported that γ-aminobutyric acid and isoflavones fortified foods can lower blood pressure. Isoflavones (natural micronutrients in vegetables), polyunsaturated fatty acids and magnesium help in the reduction of atherosclerosis and cardiovascular events [24,41]. Furthermore, mediteranean style diet pattern which contains high vegetable, fruits, nuts, whole grain, fish and low processed food is ideal in the control of most dietary related sudden unexpected natural deaths [24]. About 36.17%% (17 cases) of the victim had history of alcohol and tobacco use though the quantification was difficult as it ranged from occasional to moderate. These risk factors are important agents that accelerate atherosclerosis of blood vessels, increase the blood pressure, alter the lipid profiles and ultimately progress to cardiovascular death [42]. With the spread of malnutrition especially obesity, the prevalence of diabetes mellitus has been on the increase in Nigeria [42,43]. The prevalence of DM in Nigeria between 1963 and 1971 was less than 1% however, current reports indicate that it is between 8% and 10% [44-47]. In this study, 12.76% (6 cases) cases were hypertension co-existing with diabetes mellitus and obesity. Though DM may be a primary cause of SUND especially following its acute complications [31,48] in our observations DM was a co-morbid condition may be commoner in blacks. Reinier et al. [49] reported that African-Americans diagnosed with sudden unexpected natural death have higher prevalence of DM compared to the white counterparts. Moreover, Srivatsa et al. [48] observed that smoking, DM and obesity are important risk factors in India. Several reports indicated that diabetes mellitus, dyslipidaemia and obesity have summative adverse prognostic effect on hypertension and subsequent cardiovascular events [50-56].
The second most common cause of SUND in our study was gastrointestinal diseases which constituted 8.5% (4 cases). Majority of the gastrointestinal diseases were due to hepatic diseases especially cirrhosis with rupture of esophageal varices and perforated gastric ulcer. Reports from Benin City, Port Harcourt and Osogbo demonstrated that gastrointestinal diseases were the causes of SUND in 1.2%, 4% and 6% respectively [4,16,19]. Similarly, 6.7%, 10.7%, 13.8% of SUND in South Africa, India, Iran, and Thailand respectively were due to complications of gastrointestinal diseases [6,13,15,33]. The Central nervous system constituted 21.3% (10 cases) of all the SUND in this study. Bacterial meningitis and intracranial hemorrhage were the causes of sudden CNS-related death. The intracranial haemorrhages constituted 80% of the CNS diseases in this study with a 62.9% occurring in males. This observation agrees with previous studies [4,13,16,17,37]. However, 7.5%, 7.6%,12%,17.1% were reported in Iran, Thailand, India, South Africa respectively.13,14,6,33 In Glasgow, Black and Graham [57] reported that intracranial haemorrhage and bacterial meningitis were the second and sixth commonest cause of sudden unexpected CNS-related death respectively. The cerebrospinal bacterial meningitis may be related to ineffective phagocytosis that pave way for fulminant bacterial infection especially in patients with defective immune system [58]. However, the victims of bacterial meningitis in this study had no family or personal history of a premorbid condition that could account for the infections. The organisms isolated from the intracranial exudates were Klebsiella spp and Streptococcus spp. These organisms have special characteristics especially the protective capsules which make phagocytosis difficult and in this case no effective medical attention was sort before the death. In developed countries infective causes of CNS diseases appear to be low. For instance, Epilepsy is the commonest cause CNSrelated sudden death in Scotland and Ireland [8,57]. The eight cases with intracranial haemorrhage were known hypertensives except two cases with ruptured berry aneurysm. Bowen et al. [59] reported that in 20% of cases rupture of berry aneurysms could be sudden and unexpected.
The respiratory system contributed 4.3% (2 cases), all occurred in males. The immediate causes of death were Cor Pulmonale following chronic lung disease and aspiration of gastric content respectively. Obiora et al. [4] made similar observation in Port Harcourt. However; several reports from other parts of Nigeria showed that diseases of the respiratory system contribute a significant number to SUND. For instance, 12.5%, 18.2%, 20.7% were reported from Benin City, Ile-Ife, and Oshogbo respectively [16,17,19]. Similarly, 16.4%, 22.4%, 26%, 34.2% in Thailand, Turkey, India, South Africa respectively [6,14,18,25]. Previous studies in USA, England, France, Italy, South Africa, Germany and Wales demonstrated that acute viral infection of the respiratory tract can be a cause of sudden death especially in children below the age of six years [60-65]. In this study, the aspiration of gastric content occurred in a patient with acute alcohol intoxication. Alcohol misuse is a common cause of SUND and this usually follow acute intoxication, alcohol ketoacidosis or alcohol-induced cardiac arrhythmias [66,67].
The vascular events leading to SUND in this study were aortic dissection and pulmonary embolism. They constituted 4.3% of all the observations in our study. These were rare causes of SUND in our environment [4,16-19]. Clouse et al. [68] reported that aortic dissection is an uncommon cause of sudden death with the reported incidence of 3.5 per 100,000 annually in USA. Similar reports were made from Ireland, India, Spain, Japan and Germany [8,25,69-71]. The second vascular cause of death in this study was a case of an obese young female who died of pulmonary embolism. Though most previous studies in Nigeria had no case of pulmonary embolism as primary cause of sudden natural death, Akinwusi et al. [19] reported that 10.4% of sudden unexpected natural death in Oshogbo was caused by pulmonary embolism. Moreover, several reports demonstrated that 4.3%, 4.7%, 7.4% and 7.5% of SUND were attributable to pulmonary embolism in Spain, Jamaica, India and Iran respectively [32,72-83].
Conclusion
Finally, not all cases of sudden natural death are resolved even after extensive postmortem examination. In our study, the causes of death in 6.4% (3 cases) of the deceased were undetermined. In Ghana, Holland, Thailand, India and Australia undetermined causes of SUND accounted for 1.87%, 8.8%, 9%, 14.6% and 31% respectively. Several reports demonstrated that most unexplained deaths were mostly due to sudden primary arrhythmogenic causes in people with structurally normal hearts hence, genetic defects may be involved.
24372
References
- Steyn K, Damasceno A (2006) Lifestyle and related risk factors for chronic diseases. In: Jamison DT, Feachem RG, Makgoba MW (Eds). Disease and mortality in Sub-Saharan Africa. (2ndedn), Washington (DC): The International Bank for Reconstruction and Development / The World Bank, Chapter 18.
- Mohamed EY, Abdelbadie A, Abdalla SM, Alsideg AA, Khamis AH (2008) Sudden natural death in Khartoum Mortuary. Sudan J Med Sci 3: 319-324.
- International Classification of Diseases (ICD-10). Geneva, World Health Organization, 2005.
- Obiorah CC, Amakiri CNT (2012) Systemic Analysis of Sudden Natural Deaths at Braithwaite Memorial Specialist Hospital Port Harcourt, Nigeria. TNHJ 12: 47-51.
- Craig CH (1984) Death due to sudden or unexpected natural causes. In: Mant AK (eds). Taylor’s Principles and Practice of Medical Jurisprudence. London: Churchill Livingstone 111: 1-10.
- Udnoon J, Chirachariyavej T, Peonim V (2009) Sudden unexpected deaths in different age groups at Ramathibodi Hospital, Bangkok, Thailand: A retrospective autopsy study during 2003-2007. Southeast Asian J Trop Med Public Health 40: 162-168.
- Chugh SS, Jui J, Gunson K, Stecker EC, John BT, et al. (2004) Current burden of sudden cardiac death: multiple source surveillance versus retrospective death certificate-based review in a large U.S. community. J Am Coll Cardiol 44: 1268-1275.
- Byrne R, Constant O, Smyth Y, Callagy G, Nash P, et al. (2008) Multiple source surveillance incidence and aetiology of out-of-hospital sudden cardiac death in a rural population in the West of Ireland. Eur Heart J 29: 1418-1423.
- Zhang S (2009) Sudden cardiac death in China. Pacing Clin Electrophysiol 32: 1159-1162.
- Tokashiki T, Muratani A, Kimura Y, Muratani H, Fukiyama K (1999) Sudden death in the general population in Okinawa: incidence and causes of death. Jpn Circ J 63: 37-42.
- Papadakis M, Sharma SS, Cox S, Sheppard MN, Panoulas VF, et al. (2009) The magnitude of sudden cardiac death in the young: a death certificate-based review in England and Wales. Europace 11: 1353-1358.
- Stein C (2009) Out-of-hospital cardiac arrest cases in Johannesburg, South Africa: a first glimpse of short-term outcomes from a paramedic clinical learning database. Emerg Med J 26: 670-674.
- Chugh SS, Reinier K, Teodorescu C, Evanado A, Kehr E, et al. (2008) Epidemiology of sudden cardiac death: clinical and research implications. Prog Cardiovasc Dis. 51: 213-28.
- Tiemensma M, Burger EH (2012) Sudden and unexpected deaths in an adult population, Cape Town, South Africa, 2001-2005. S Afr Med J 102: 90-94.
- Ashwinikumar S, Madhusudan P, Ajay G, Praveen A, Sandesh D (2015) Autopsy profile of natural causes of sudden deaths and survival time. IJHBR 3: 126-134.
- Ugiagbe EE, Ugiagbe RA (2012) Causes of sudden natural death: a medicolegal autopsy study of medical cases in an African referral center. East Afr Med J 89: 332-338.
- Pelemo OE, Sabageh D, Komolafe AO, Sabageh AO, Odesanmi WO (2014) An autopsy review of sudden unexpected natural deaths in a suburban Nigerian population. Popul Health Metr 12: 26.
- Nnoli M, Charles NC, Omotoso AJ, Ogbonna NC (2014) Sudden deaths in hotels following sexual intercourse at southeastern Nigeria from 2010 to 2013. Afr J Med Health Sci 13: 30-33.
- Akinwusi PO, Komolafe AO, Olayemi OO, Adeomi AA (2013) The pattern of sudden death at Ladoke Akintola University of Technology Teaching Hospital, Osogbo, South West Nigeria. Vasc Health Risk Manag 9: 333-339.
- Ngbea JA, Vhriterhire RA, Okani CO, Echekwube PO, Nyaga T, et al. (2017) An autopsy review of sudden unexpected natural deaths at Benue State University Teaching Hospital, Makurdi, North Central, Nigeria. Ann Trop Pathol 8: 112-115.
- Federal Republic of Nigeria Official Gazette (2007) "Legal Notice on Publication of the Details of the Breakdown of the National and State Provisional Totals 2006 Census" (PDF). Archived from the original (PDF) on 2007-07-04.
- Acholonu ADW (2008) Water quality studies of Nworie River in Owerri, Nigeria". Mississippi Academy of Sciences.
- Hayashi M, Shimizu W, Albert CM (2015) The spectrum of epidemiology underlying sudden cardiac death. Circ Res 116: 1887-1906.
- Ozdemir B, Celbis O, Onal R, Mizrak B, Karakoc Y (2012) Multiple organ pathologies underlying in sudden natural deaths. Med Sci 1: 13-26.
- Morentin B, Audicana C (2011) Population-based study of out-of-hospital sudden cardiovascular death: incidence and causes of death in middle-aged adults. Rev Esp Cardiol 64: 28-34.
- Chaturvedi M, Satoskar M, Khare MS, Kalgutkar AD (2011) Sudden, unexpected and natural death in young adults of age between 18 and 35 years: A clinicopathological study. Indian J Pathol Microbiol 54: 47-50.
- Zheng Z, Croft JB, Giles WH, Mensah GA (2001) Sudden cardiac death in the United States, 1989 to 1998. Circulation 104: 2158-2163.
- Hua W, Zhang L, Wu Y, Liu X, Guo D, et al. (2009) Incidence of Sudden Cardiac Death in China; Analysis of 4 Regional Populations. JACC 54: 1110-1118.
- Gurger M, Turkoglu A, Atescelik M, Bork T, Tokdemir M, et al. (2014) Sudden Suspected Death in Emergency Department: Autopsy Results. Turk J Emerg Med 14: 115-120
- Nofal HK, Abdulmohsen MF, Khamis AH (2011) Incidence and causes of sudden death in a university hospital in eastern Saudi Arabia. EMHJ 17: 665-670.
- Rao D, Sood D, Pathak P, Dongre SD (2014) Cause of sudden cardiac deaths on autopsy findings; a four-year report. Emerg 2: 12-17.
- Fayaz AF, Goudarzi A, Taghaddosinejad F, Behnoush B (2015) Sudden Unexpected Natural Death in the Youth; an Iranian Single Center Investigation. IJMTFM 5: 8-11.
- Tavora F, Zhang Y, Zhang M, Li L, Ripple M, et al. (2012) Cardiomegaly is a common arrhythmogenic substrate in adult sudden cardiac deaths, and is associated with obesity. Pathol 44: 187-191.
- Carnethon MR, Pu J, Howard G, Albert, Anderson CAM, et al. (2017) Cardiovascular health in African Americans a scientific statement from the American Heart Association. Circulation 136: 1-10.
- Anderson RE, Hill RB, Broudy DW, Key CR, Pathak D (1994) A population-based autopsy study of sudden, unexpected deaths from natural causes among persons 5 to 39 years old during a 12-year period. Human Pathol 25: 1332-1340.
- Pandian JR, Laishram RS, Kumar LD, Phuritsabam P, Debnath K (2014) Autopsy review of sudden deaths in a tertiary hospital in northeastern India. J Med Soc 28: 145-148.
- Bowker TJ, Wood DA, Davies MJ, Sheppard MN, Cary NRB, et al. (2003) Sudden, unexpected cardiac or unexplained death in England: a national survey. Q J Med 96: 269-279.
- https://www.fao.org/nutrition/education/food-dietary-guidelines/regions/countries/nigeria/en/
- Nishimura M, Yoshida S, Haramoto M, Mizuno H, Fukuda T, et al. (2016) Effects of white rice containing enriched gamma-aminobutyric acid on blood pressure. J Tradit Complement Med 6: 66-71.
- Fayed AE (2015) Review article: health benefits of some physiologically active ingredients and their suitability as yoghurt fortifiers. J Food Sci Technol 52: 2512-2521.
- Wakabayashi I (2011) Combined impact of alcohol and tobacco: implications for cardiovascular disease. Curr Cardiovasc Risk Rep 5: 501.
- Akinkugbe OO (1997) Non-communicable diseases in Nigeria: National Survey (Final report) on Hypertension, Coronary Heart Disease, Diabetes Mellitus, Haemoglobinopathies, G6PD deficiency and Anaemia. National Expert Committee on Non-Communicable Disease. Lagos, Nigeria: Federal Ministry of Health and Social Services.
- Olatunbosun ST, Ojo PO, Fineberg NS, Bella AF (1998) Prevalence of diabetes mellitus and impaired glucose tolerance in a group of urban adults in Nigeria. J Natl Med Assoc 90: 293-301.
- Erasmus RT, Fakeye T, Olukoga O, Okesina AB, Ebomoyi E, et al. (1989) Prevalence of diabetes mellitus in a Nigerian population. Trans R Soc Trop Med Hyg. 83: 417-418.
- Ogbera AO, Ekpebegh C (2014) Diabetes mellitus in Nigeria: The past, present and future. World J Diabetes 5: 905-991.
- Srivatsa UN, Swaminathan K, Munavarah KSA, Amsterdam E, Shantaraman K (2016) Sudden cardiac death in South India: Incidence, risk factors and pathology. Indian Pacing Electrophysiol J 16: 121-125.
- Reinier K, Nichols GA, Huertas-Vazquez A, Uy-Evanado A, Teodorescu C, et al. (2015) Distinctive clinical profile of blacks versus whites presenting with sudden cardiac arrest. Circulation 132: 380-387.
- Adabag S, Huxley RR, Lopez FL, Chen LY, Sotoodehnia N, et al. (2015) Obesity related risk of sudden cardiac death in the atherosclerosis risk in communities study. Heart 101: 215- 221.
- Plourde B, Sarrazin JF, Nault I, Poirier P (2014) Sudden cardiac death and obesity. Expert Rev Cardiovasc Ther 12: 1099-1110.
- Perju-Dumbrava D, Chiroban O, Radu CC (2017) Obesity and Overweight Risk Factors in Sudden Death Due to Cardiovascular Causes: A Case Series. Iran J Public Health 46: 856-857.
- Giday A, Wolde M, Yihdego D (2010) Hypertension, obesity and central obesity in diabetics and non-diabetics in Southern Ethiopia. Ethiop J Health Dev 24: 145-147.
- El-Atat FA, McFarlane SI, Sowers JR, Bigger JT (2004) Sudden cardiac death in patients with diabetes. Current Diabetes Reports 4: 187-193.
- Curb JD, Rodriguez BL, Burchfiel CM, Abbott RD, Chiu D, et al. (1995) Sudden Death, Impaired Glucose Tolerance, and Diabetes in Japanese American Men. Circulation. 91: 2591-2595.
- Lewis ME, Lin FC, Nanavati P, Mehta N, Mounsey L, et al. (2016) Estimated incidence and risk factors of sudden unexpected death. Open Heart 3: e000321.
- Black M, Graham DI (2002) Sudden unexplained death in adults caused by intracranial pathology. J Clin Pathol 55: 44-50.
- Tajiri T, Tate G, Miura K, Masuda S, Ohike N, et al. (2008) Sudden death caused by fulminant bacterial infection: background and pathogenesis of Japanese adult cases. Intern Med. 47: 1499-1504.
- Bowen DAL (1984) Ruptured berry aneurysms: A clinical, pathological and forensic review. Forensic Sci Int 26: 227-234.
- Moore C, Bamber A, James R, Jones R (2005) Respiratory viruses and sudden death – Cause or innocent bystanders? J Clin Virol 70: S1-S126.
- Desmons A, Terrade C, Boulagnon C, Giusti D, Nguyen Y, et al. (2013) Post-mortem diagnosis, of cytomegalovirus and varicella zoster virus co-infection by combined histology and tissue molecular biology, in a sudden unexplained infant death. J Clin Virol 58: 486-489.
- Burger MC, Dempers JJ, de Beer C (2014) Profiling the approach to the investigation of viral infections in cases of sudden unexpected death in infancy in the Western Cape Province, South Africa. Forensic Sci Int 239: 27-30.
- Weber MA, Hartley JC, Ashworth MT (2010) Virological investigations in sudden unexpected deaths in infancy (SUDI). Forensic Sci Med Pathol 6: 261-267.
- Lucas JR, Haas EA, Masoumi H (2009) Sudden death in a toddler with laryngotracheitis caused by human parainfluenza virus-1. Pediatr Dev Pathol 12: 165-168.
- Dettmeyer R, Sperhake JP, Müller J (2008) Cytomegalovirus-induced pneumonia and myocarditis in three cases of suspected sudden infant death syndrome (SIDS): diagnosis by immunohistochemical techniques and molecular pathologic methods. Forensic Sci Int 174: 229-233.
- Templeton AH, Carter KLT, Sheron N, Gallagher PJ, Verrill C (2009) Sudden Unexpected Death in Alcohol Misuse-An Unrecognized Public Health Issue? Int J Environ Res Public Health 6: 3070-3081.
- Komarekova I, Novomesky F, Straka L (2014) The Fatal Alcoholic Ketoacidosis as a Dilemma in the Differential Diagnosis in Unexpected Deaths. J Forensic Sci Criminol 2: 101.
- Clouse WD, Hallett JW Jr, Schaff HV, Spittell PC, Rowland CM, et al. (2004) Acute aortic dissection: population-based incidence compared with degenerative aortic aneurysm rupture. Mayo Clin Pro 79: 176-180.
- Rastogi P, Kanchan T (2014) Acute aortic dissection – A rare cause of sudden death. J Punjab Acad Forensic Med Toxicol 14: 119-120.
- Chiba T, Nishida N, Ohtani M, Suzuki I, Yoshioka N (2006) Fatal hemopericardium caused by retrograde acute abdominal aortic dissection: an autopsy report and morphological consideration. Int J Cardiol 112: 253-255.
- Jungmann L, Bohnert M, Schmidt U, Pollak S (2010) Sudden/unexpected death due to spontaneous aortic rupture: two unusual manifestation forms. Arch Kriminol 226: 55-65.
- Lucena J, Rico A, Vázquez R, Marín R, Martínez C, et al. (2009) Pulmonary embolism and sudden-unexpected death: prospective study on 2477 forensic autopsies performed at the Institute of Legal Medicine in Seville. J Forensic Leg Med 16: 196-201.
- Escoffery CT, Shirley SE (2002) Causes of natural death in Jamaica: a medicolagal (autopsy) study from university of West Indies. Forensic Sci Int 129: 116-121.
- Rao DS, Yadhukul S (2008) Sudden and unexpected natural deaths - a four-year autopsy review. JPAFMAT 8: 20-24.
- Vander-Geest S (2004) Dying peacefully: considering good death and bad death in Kwahu-Tafo, Ghana. Soc Sci Med 58: 899-911.
- Doolan A, Langlois N, Semsarian C (2004) Causes of sudden cardiac death in young Australians. Med J Aust 180: 110-112.
- Vaartjes I, Hendrix A, Hertogh EM, Grobbee DE, Doevendans PA, et al. (2009) Sudden death in persons younger than 40 years of age: incidence and causes. Eur J Cardiovasc Prev Rehabil 16: 592-596.
- Wever EFD, Robles de Medina EO (2004) Sudden Death in Patients without Structural Heart Disease. J Am Coll Cardiol 43: 1137-1144.
- Doolan A, Langlois N, Semsarian C (2004) Causes of sudden cardiac death in young Australians. MJA 180: 110-112.
- Hookana E, Junttila EJ, PuurunenVP, Tikkanen JT, Kaikkonen KS, et al. (2011) Causes of non-ischemic sudden cardiac death in the current era. Heart Rhythm 8: 1570-1575.
- Fernandez-Falgueras A, Sarquella-Brugada G, Brugada J, Brugada R, Campuzano O, et al. (2017) Cardiac channelopathies and sudden death: recent clinical and genetic advances. Biol 6: 1-21.
- Lim Z, Gibbs K, Potts JE, Sanatani S (2010) A reviews of sudden unexpected death in the young in British Columbia. Can J Cardiol 26: 22-26.
- Katritsis DG, Gersh BJ, Camm AJ (2016) A clinical perspective on sudden cardiac death. Arrhythm Electrophysiol Rev 5: 177-182.

