Asha Pratinidhi1*, Rajkumar Patange2, Supriya Patil3, Jyoti Salunkhe4, Sheetal Samson4, Satish Kakade5
1Research Director, MD (Preventive & Social Medicine), DPH, DCH, Krishna Institute of Medical Sciences Deemed University, Karad
2M.D. Professor, Head of Department, Obstetrics and Gynecology,Department Krishna Hospital, Karad
3RN, RM, M.Sc Nursing Associate Professor Krishna Institute of Nursing Sciences, Karad
4M.Sc PhD, Associate Professor, Department of Preventive & Social Medicine Krishna Institute of Medical Sciences Karad
- *Corresponding Author:
- Asha Pratinidhi
Research Director
Krishna Institute of Medical Sciences Deemed University
Karad, Maharashtra, India
E-mail: ashapratinidhi@gmail.com
Keywords
Simulation, training device, cervical dilatation, partograph, cervicograph
Introduction
Two skills are used for clinical monitoring of progress of labour namely abdominal palpation and vaginal examination, out of which vaginal examination is the most accepted method of measuring progress of labor. There are six important parameters of progress of labor namely anterior movement effacement, ripening, dilatation of cervix and rotation, flexion & moulding of fetal head and the descent [1]. Vaginal examination uses two objective criteria to assess progress of labour, cervical dilatation and descent of fetal presenting part. Assessment of cervical dilatation in centimeter is one of the most important aspect of vaginal examination during labour. There are very few studies evaluating the ability of birth attendants to judge the cervical dilatation [2,3]. There is a lot of inter observer variation. Conventionally cervical dilation is stated in terms of fingers.
The size of the fingers vary and so also the number of fingers expressing cervical dilatation. Knowledge of cervical dilatation in centimeters is an essential pre requisite of plotting of cervicograph. Cervicograph is an important component of partograph which is recommended by WHO for monitoring of every delivery [4]. Cervicographic monitoring of labour can detect delayed progress timely for augmentation and referral of delivering woman for appropriate intervention [5]. There are many reasons why inspite of recommendation of WHO6and training received by nursing staff under RCH II programme the use of the partography including cervicography is not routinely undertaken.
Thus there are two main hurdles in using cervicograph namely assessment of size of cervix in centimeters & ploting of cervical dilatation in relation to duration of labour.
In India majority of the deliveries are conducted by ANMs in rural areas & nurse midwives in urban hospitals. That is the reason for all four courses in nursing namely Revised General Nursing and Midwifery, Post Basic B Sc Nursing, Basic B Sc Nursing and M Sc Nursing in India includes midwifery as one of the compulsory subjects. While they are posted in obstetrics wards by rotation for a total period of five and half months, each one of them has to conduct 20 deliveries under supervision. By the time they became graduates & start doing internship they are well-versed with the stages and phases of delivery and are expected to know the cervical dilatation. That is the reason why we decided to test simulation training device on bachelor of nursing students, while they were posted for internship. Utility of simulation training device over and above conventional training was tested on a batch of students during internship period after completion of midwifery undergraduate training and presented in this paper.
Materials and Methods
The simulation training device for assessment of cervical dilatation comprises of supporting platform for supporting the components of the device and a rotating plastic drum which is closed on both sides by plastic discs. The plastic discs are glued to the rotating drum and are connected to a shaft. The rotating drum is rigidly connected to the shaft and has a plurality of rubber-lined holes of varying diameters. A box covers the rotating drum and has an opening which is selectively coverable by an opaque cloth or a curtain. The device further includes an indexing mechanism, a turn wheel and a scale. The indexing mechanism has a spring- loaded lock and a slotted indexing wheel, wherein the slotted indexing wheel is fixed to the shaft and allows the rotating drum to rotate in one direction. The turn wheel is mounted on the shaft and has an indication arrow. With the help of wheel one ring at a time of desired size can be positioned in the center of the opening of the box. (Fig 1) The trainee student has to learn to judge the diameter of the holes by visual impression and palpation. After gaining confidence of his or her jugdement of cervical dilation by using the simulation device while the curtain is off, the curtain is put on for blind palpations on the device. When this skill is acquired the trainee is ready for performing examinations on human patients.

Figure 1: Simulation Model
A comparative study of correct assessment of size of the hole from 3 cm diameter to 10 cm diameter (3-10 cm) was undertaken on 7-9-2011 at Krishna Institute of Nursing Sciences, Karad. One batch of 100 students of 4th year Basic B. Sc nursing was randomly allocated to study and control groups. 12 students were absent on that day thus 88 students participated in the study.
A special lecture was arranged for these students to highlight the importance of measurement of cervical dilatation during labour, anatomy of cervix, stages and phases of labour, cervicography and partographic monitoring of labour. Fourth year Basic B.Sc nursing students are well versed with the management of labour and are routinely conducting the deliveries under the guidance of an obstetrician.
The knowledge of participants from both the groups (study=43) (control=45) was tested by a pre-tested questionnaire. The questionnaire consisted of the questions related to the cervicograph and partograph. One mark was given for correct answer for a question, no negative marking was done. Same performa was used for assessment of post training scores.
After demonstration of working of this model it was left to the student for practicing visual and tactile assessment of the size of inner diameter of the rubber rings.
For evaluation of correctness of assessment of size of the hole, the curtain was placed to blind the student being tested. The control group (n=45) was given training as was given routinely for the batch of nursing students. Thus the study group received routine training and training on simulation model and control group received only routine training. Assessment was undertaken individually with the help of simulation model after blinding. SPSS version 20 was used for statistical analysis.
Unpaired‘t’ test was used to compare pre and post test knowledge between the study and control groups. X2 test was used to compare ability of each nursing student to identify correctly the size of the hole of the rubber rings after blinding. (Fig. 1)
Results
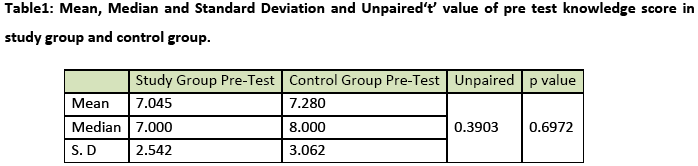
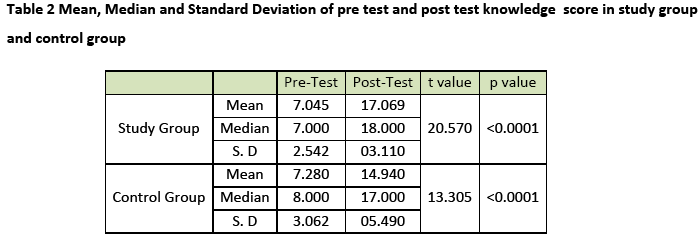
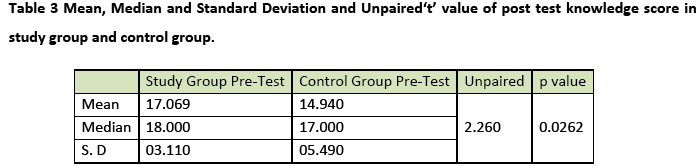
The knowledge of students in study and control group revealed a pre-training mean score of 7.045 for study group and 7.28 for control group. The difference was not statistically significant. There was no significant difference in the pre test scores of study and control group.(Table 1). Though the post test scores improved significantly in both the groups the increase was significantly more in the study group as compared to control group. (Table 2) Individualized assessment of judgment on simulation training device indicated a highly significant ability of the nursing student from study group as compared to control group in judging and interpreting the size of the hole (Table 3).
All the skills shown in the table 4. were significantly better in study group as compared to the control group. (Table 4)

Feedback
The participants from study group who were using this simulation training device thought that it was a unique experience and it definitely improved their understanding about assessment of ring size in centimeter.
Discussion
Cervical dilatation is enlargement of the cervical of opening (os) from 0-10 cm. Nurses should know how to assess correct dilation of cervix of delivering women. By the use of simulation training device in addition to conventional training, the study group did improve the judgment of size of the ring significantly as compared to the control group, where only conventional training was given. The ability of participants from study group was better for identification of correct size of the given ring by visual impression, as well as by the tactile sensation.
Graphic analysis of labour was published by Fridmen [7] in 1954. Bachmann Libhaber [2] performed independent cervical assessment. The assessment used as standard was performed by the experience of obstratic consultant (Researcher) and other assessment was done by consultants & regisisters at various level of training. There was 49.2 % agreement & 11% differed by 2cm. or more. Accuracy was low at 3 to 4 cm. cervical size & higher at 8 to 10 cm. Size. It was observed in present study that 8 (18.6%) from study group & 22 (48.9%) from control group wrongly stated the cervical diameter at the time of assessment. There were more mistakes when the dilation was beyond 4 fingers roughly corresponds to 5 cm. & above since the birth attendant are accustomed to judge cervical dilatation in fingers and then convert into centimeters.
A comparison of clinical assessment of ultrasonographic assessment of size of cervix was under taken by Zimerman et al., [8] carried out study on 52 patients and found out that assessment of cervical dilatation using 3D ultrasonography during labour is feasible and reproducible.
Ultrasonographic measurements & digital vaginal examinations showed a possible correlation. Ultrasonograhic findings are more objective but it can not be undertaken routinely in India for labouring women. We have conducted in vitro assessment of size of ring.
Robson [9] studied 52 participants (midwives, doctors, student midwives & medical students) using simulation model also found significant variation in estimation of effacement & dilatation. Because of possibility of intra observer variation & inaccuracy, Clement [10] has recommended that vaginal examinations should be carried out by the same midwife where possible. A carefully designed set of simulators showing cervical effacement & dilatation was used by Tufnell DJ et al. [3] Error within & between observers was assessed in 36 midwives and 24 obstetricians, no observer was correct in every case and there was no significant difference between the two groups. Inaccuracies were gratestest at 5 to 7cms of dilatations. The findings of our study are similar that inaccuracy in assessment was more after 5cm cervical dilatation. Conventionally, assessment of cervical dilatation of a patient is first performed by a teacher in obstetrics and gynecology, and then the teacher informs the students of the size of the cervix just examined by him. Next, the student is asked to perform an internal examination of the patient. The student must then commit to memory the relationship between the examination just performed and the particular cervical dilatation size of which he /she has been informed.
Such conventional training techniques transfer the subjective impression of one person to another person without facilitating visual guidance about the actual cervical dilation size. Each and every student of medicine and nursing has to undergo such training without facilities (e.g. a dummy model) for forming their own judgment. Such conventional training technique is far from perfect and is likely to result in gaps in a student’s training, such that the student is likely to have inaccurate judgment of the cervical dilatation assessments. Also, when a series of students palpate the patients internally as a part of training or teaching exercise, there is not only a risk of infection to the patient due to repeated internal examinations, but also a risk of psychological trauma and of the physical discomfort. These ethical issues will be minimized by use of simulation training device. The simulation training device was developed during a project under taken to use colour coded rings by nurse midwives [11] supported by Government of India. It was pretested in the field but was not tested on the nursing students with an objective of introducing it as a training device at nursing colleges. The results of this study are encouraging.
It is not expected that this simulation device will mimic the situation of cervix in vivo but would give visual and palpatory learning experience to nursing students about the size of the cervix. This can be considered as in vitro training device to improve understanding of the students about cervical size so that minimum number of examinations and time will be required on live subjects for development of accurate skill of judgment of size of cervix in centimeters.
Since this simulation training device is newly invented one, there are no previous studies for comparison. The feedback from the participant students from the study group was uniformly favorable. The student have feeling a that, the device helped them in better understanding of the cervical dilatation in centimeters and their ability to visualize the size of expected cervical dilation at the end 4 hours period before recommended second vaginal examination. They are confident to plot the cervicograph. It is therefore recommended that, the simulation training device for assessment of cervical dilatation is a useful device which can be used routinely in the training of birth attendants for betterment of skill development in the area of judgment of cervical dilatation. Visual impression of the ring size and its palpatory feel together improve the understanding of the students. Use of simulation training device could be a valuable addition in the routine nursing teaching programme.
2624
References
- Simkin P and Ancheta R The Labour Progress Handbook: Early Interventions to Prevent and Treat Dystocia Ed.,Wiley-Blackwell Science, Oxford 2000.
- Buchmann EJ, Libhaber E. Accuracy of cervical assessment in the active phase of labour. BJOG 2007; 114(7):833-7.
- Tufnell DJ, Bryee F, Johnson N, Lilford RJ. Simulation of cervical changes in labour: reproducibility of expert assessment. The Lancent 1989; 2(8671):1089-90.
- Website: Introduction to assessment of progress in labour. Available from https://www.rcog.org.uk/stratog/page/introduction-assessment-progress-labour. Accessed on 14thDec 2013.
- Website: The Partrograph: An Essential Tool for Decision-Making during labour. Available from https:// pdfdocs / PNACT 388. Accessed on 14thDec 2013.
- World Health Organization Maternal Health and Safe Mother Hood Programme. Lancet 1994;343(8910):1399-404
- Freidmen EA. The Graphic Analysis of labour. American Journal Obstetrics and Gynecology 1954; 68(6):1568-1575.
- Zimermen AL, Smolin A, Maymom R, Weinraub Z, Herman A , Tobvin Y. Intrapartum mearsument of cervical dilatation using translabial 3- dimensional ultrasonography: correlation with digital examination and interobserver and intraobserver agreement assessment. J Ultrasound Med 2009;28(10):1289-96.
- Robson S. Variation of Cervical dilatation estimation estimation by midwives, doctors, student midwives and medical students in 1985 ? a small study using cervical simulation models. Research and the Midwife Conference Proceedings Manchester, University of Manchester,1991.
- Clement S. Unwanted vaginal examinations. British Journal of Midwifery 1994; 2(8): 368-370.
- Pratinidhi AK, Javadekar SS, Shrotri AN, Gandham SV, Patil A, Patil KS. Feasibility of use of color-coded rings by nurse midwives: an appropriate technology based on partographic principles. Indian J Community Med 2013; 38(3):157-61.

