Khaira Boussouf1,3, Zoubida Zaidi2,3*, Sara Soltani1, Fatima Kadour1,3and Azouz Djellaoudji1,3
1Department of Cardiology, University Hospital of Setif, Algeria
2Department of Epidemiology, University Hospital of Setif, Algeria
3Genetic and Nutritional Cardiovascular Diseases Laboratory, Medical Faculty of Setif, University Ferhat Abbas, Setif, Algeria
*Corresponding Author:
Zoubida Zaidi
Department of Epidemiology
University Hospital of Setif
Algeria
Tel: 00213561728758
E-mail: zozaidi@yahoo.fr
Received date: 01 January 2019 ; Accepted date: 05 February 2019; Published date: 12 February 2019
Citation: Boussouf K, Zaidi Z, Soltani S, Kadour F, Djellaoudji A (2019) Tetralogy of Fallot in Four Down Syndrome Patients in Setif, Algeria: Diagnosis and Clinical Aspects. Health Sci J Vol.13.No.1:629.
Copyright: © 2019 Boussouf K, et al. This is an open-access article distributed under the terms of the creative commons attribution license, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Keywords
Down syndrome; Tetralogy; Congenital heart disease
Introduction
The Tetralogy of Fallot (TF) is by far the most common cyanogenic Congenital Heart Disease (CHD) and represents 75% in the general population [1,2], it has a broad anatomical spectrum. In the mild forms, the obstruction is located only at the level of the right ventricular infundibulum whereas in the severe forms, the pulmonary valve is atretic, the pulmonary arteries are absent and the pulmonary irrigation is done by collateral aorto-pulmonary [3-6]. The etiology is multifactorial, but the disease has been reported related to untreated maternal diabetes, phenylketonuria and retinoic acid consumption. Associated chromosomal abnormalities may include trisomies 21, 18 and 13.
Trisomy 21 (T21) is the most frequent of these chromosomal aberrations, it is characterized by a dysmorphic syndrome, a mental retardation more or less deep, and y frequently associated with (CHD) [7-9]. The TF represents according to the statistics 5%-8% of all CHDs in T21 [10,11].
The purpose of this study is to describe four cases of this CHD among patient with down syndrome.
Patients and Methods
Patients with CHD were examined in 06 medico-educational centers and in the department paediatric of the UHS. Information was collected on the age of the mother, the degree of parental consanguinity, the age and sex of the patient. All patients had a clinical examination, a chest X-ray, an electrocardiogram and echocardiography, the type of cardiac malformation and associated extra-cardiac abnormalities were eventually done. Patients with Down syndrome are clinically diagnosed by the presence of a characteristic pheno- type confirmed by chromosome analysis.
Statistical Analysis
The calculations were carried out by the software Epi-info version 6 produced by the Centers for Disease Control and Prevention (CDC). For quantitative variables, means and standard deviations were calculated with their 95% confidence intervals. Discrete variables are presented in number and percentage. For all analyzes, a value of p<0.05 was considered statistically significant.
Results
One hundred and ten Trisomy 21patients with CHD were included.
The most common CHD was the Atrioventricular Septal Defect (AVSD) with a frequency of 44.5% followed by Ventricular Septal Defect (VSD). The TF accounted for 3.6% of cases (Figure 1), the average age of patients was 3 years with extremes ranging from 4 months 9 years with a sex ratio is 1.
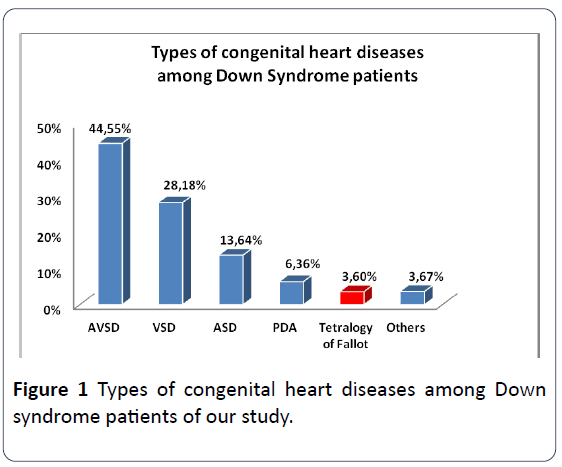
Figure 1: Types of congenital heart diseases among Down syndrome patients of our study.
AVSD: Atrioventricular Septal Defect, VSD: Ventricular Septal Defect, ASD: Ventricular Septal Defect, PDA: Persistent Ductus Arteriosus, TF: Tetralogy of Fallot.
The results of chromosomal analysis revealed pure trisomy 21 karyotype in 81.2%, mosaic trisomy karyotype in 12.5% and translocation karyotype in 6.2%.
Of the 110 patients, the maternal age is between 21 and 49 years and an average of 36, 61.
The consanguinity of the parents when they are cousins of first degree was found in 7%.
A typical auscultation of pulmonary narrowing in all patients.
The cyanosis is of variable degree, clear in one of our patients hardly visible on the integuments but net on the lips, the tongue and the nose (Figure 2) to exaggerate during the crying, and the saturation goes from 76% to 66% with state agitation with a clubbing digital.
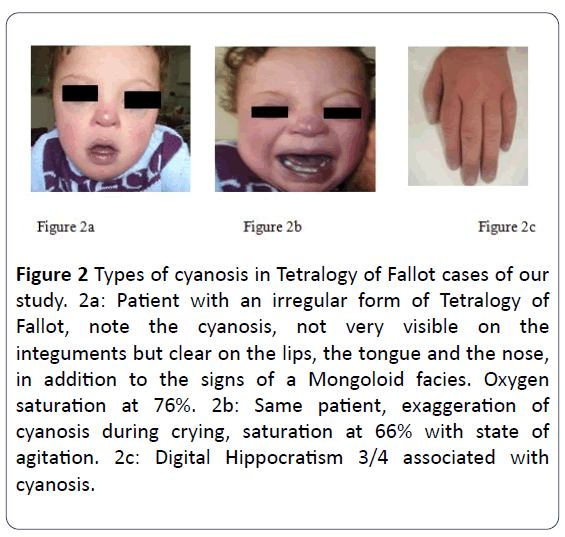
Figure 2: Types of cyanosis in Tetralogy of Fallot cases of our study. 2a: Patient with an irregular form of Tetralogy of Fallot, note the cyanosis, not very visible on the integuments but clear on the lips, the tongue and the nose, in addition to the signs of a Mongoloid facies. Oxygen saturation at 76%. 2b: Same patient, exaggeration of cyanosis during crying, saturation at 66% with state of agitation. 2c: Digital Hippocratism 3/4 associated with cyanosis.
Anoxic discomfort has been reported in two patients. Digestive abnormalities like Hirschprung's disease shown in one patient with hypothyroidism noted in a patient (Table 1).
Table 1 Distribution according to extracardiac anomalies.
| Extracardiac anomaly |
Tetralogy of Fallot |
Other CHD |
| 4 cases |
106 cases |
| Thyroid |
1 |
11 |
| Haematological |
- |
2 |
| Renale |
- |
2 |
| Orthopedic |
- |
1 |
| Digestive |
1 |
6 |
| Neurological |
- |
2 |
| Oculaire |
1 |
5 |
Our exam with the electrocardiogram shows conduction disturbances observed were of the right bundle branch type in 25% of cases, associated with signs of right ventricular hypertrophy in all patients an anovoid heart with hoof appearance by elevation of the right ventricle in two patients in chest radiography.
Echocardiography is considered to be an accurate diagnostic tool [12] by showing the anatomical elements of the disease (high AVSD, aortic dextroposition, right ventricular hypertrophy and pulmonary stenosis) (Figure 3), it also makes it possible to measure the size of the confluent branch pulmonary. Three cases of TF with hypoplasia of the pulmonary Figure 3, the coronary ostia were poorly visualized in 02 cases.
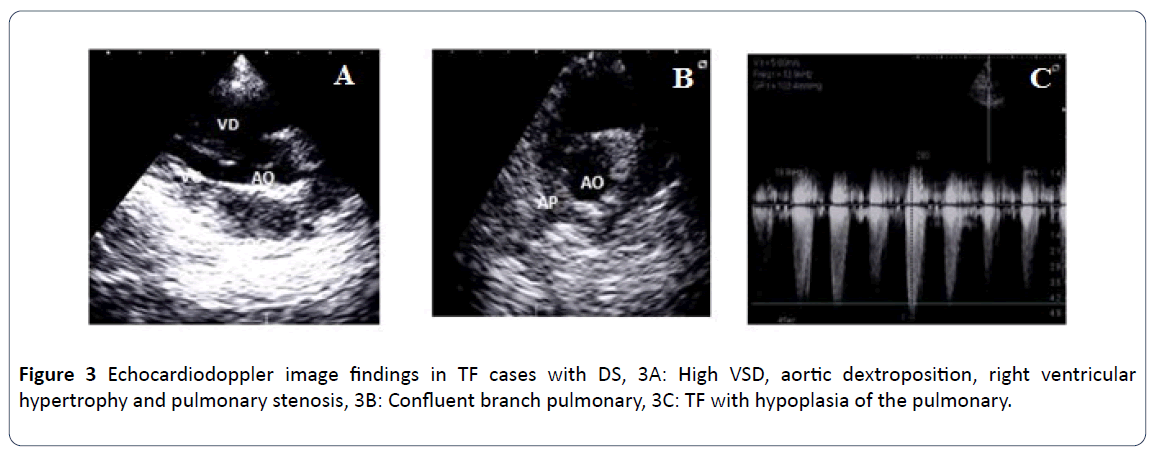
Figure 3: Echocardiodoppler image findings in TF cases with DS, 3A: High VSD, aortic dextroposition, right ventricular hypertrophy and pulmonary stenosis, 3B: Confluent branch pulmonary, 3C: TF with hypoplasia of the pulmonary.
Endocavitary exploration by cardiac catheterization was performed in two patients, the irregular forms of TF was confirmed with hypoplastic pulmonary arteries. A prophylactic treatment of anoxic discomfort with propranolol iron replacement therapy on outcomes in cardiac surgery [13,14].
In our sample, for those patients with an indication for surgery are four but who were operated is two patients, a palliative operation and a radical cure in a private clinic. Our 2 patients were followed for 18 months, a regression of cyanosis and decrease of anoxic discomfort in the patient who has benefited from palliative treatment. The evolution was good, despite the fact that a small inter-ventricular shunt with a very low flow rate and a pulmonary gradient at after the surgical treatment. No complications occurred during the controls including no stroke or infective endocarditis. On the other hand, for the patients having a surgical indication but were not operated are two, they are issued from the low socioeconomic level and the pier and postoperative risk of these patients who have a delay of healing and pulmonary infections (recused by the surgeons).
One patient died with a tetralogy of irregular Fallot with Hirschprung disease repeatedly operated for colostomy and pocket placement.
Discussion
Tetralogy of Fallot is by far the most common cyanogenic CHD, approximately 75% in the general population, and represents statistically 5% to 8% of all CHD in Trisomy 21 [1] close to the rate found in our series 3.6%. In the absence of systematic screening of CHD in the DS in our country, our patients are discovered with pulmonary regurgitation, a frequent late or accidental consequence or in an incidental finding.
Operative or catheter interventional therapy for these patients may be more complex than if the problem had been addressed in early and may have to be combined with complications.
The age of discovery varies from birth to one month. No difference in the distribution by sex in our series. A male predominance is found in other series [15,16] with a proportion of 109 (61%) boys. The poor clinical tolerance (dyspnoea, cyanosis, anoxic malaise) is significantly correlated with the irregular form of TF, the association with gastrointestinal abnormalities is already noted by several authors [17,18]. This association is due to the common origin of the digestive tract and the cardiac bulb. From a therapeutic point of view, medical treatment or palliative surgery is of great importance in relieving hypoxia and developing the pulmonary artery. Radical surgery has made decisive progress in recent years, with a mortality frequency of 4% to 10%. In terms of prognosis, in the study [15,16] show that the 178 T21 carriers of TF had a complete repair. The mortality was 4%, increased rate in comparison with that of TF without trisomy 21 (p-value 0.02). Postoperative complications (especially respiratory) and prolonged hospital stay were more common in the T21 group versus the second group of non-trisomic with TF.
In our series, only two patients underwent a complete course of treatment, the postoperative course was uncomplicated, the patient was asymptomatic without a disturbance of the ECG rhythm, but kept a residual shunt and a gradient on the pulmonary valve, nevertheless the number relatively small number of children in this group cannot be concluded and significant.
Thus for Friedli [18] study "The repair of the Tetralogy of Fallot can never restore a normal heart but it radically transforms the prognosis of this malformation", Cohen [19] Legloan et al. [20] are of the same opinion and they confirmed the majority of patients, even those who have benefited from the most refined techniques of surgery and protection myocardial, do not have a normal heart and may suffer from variable disorders in their onset, clinical manifestations and severity.
Conclusion
Our study confirmed that the profile and type of CHDs in DS in the Algerian context exhibited slight differences in the distribution of these CHDs compared with its Western countries.
With early diagnosis followed by appropriate surgical treatment, our patients who have tetralogy of Fallot live relatively normal lives, though they'll need regular medical care throughout life and might have restrictions on exercise.
Anticipation of and early implementation of prevention and treatment measures may help to reduce these post-operative morbidities in patients with Down syndrome undergoing congenital heart surgery.
24085
References
- Anderson RH, Shinebourne EA, McCarthney FJ, Tynan M (1987) Pediatric cardiology. Churchill Livingstone. London, 6: 765-798.
- Fudge JC, Shuang L, Jaggers J, O'Brien SM, Peterson ED, et al. (2010) Clinical Database Congenital Heart Surgery Outcomes in Down Syndrome: Analysis of a National. Pediatrics 126: 315-322.
- Cloarec S, Magontier N, Vaillant MC, Paillet C, Chantepie A (1999) Prevalence and distribution of congenital heart disease in Indre et Loire. Evaluation of the antenatal diagnosis (1991-1994). Arch Pediatr 6: 1059-1065.
- Veranat P, Leiva A (1986) Congenital heart disease. Encyclo Med Chir Cardiol (Paris-France) 10: 56-60.
- Dor X, Corone P (1992) Cardiac Embryology. Malformation Encyclo Medico-Chirur Cardiology 11001-C-30.
- Gay C (1998) Epidemiology, diagnosis, evolution, the review of the practitioner (Paris). 48: 999-1002.
- Barlow GM, Chen XN, Shi ZY, Lyons GE, Kurnit DM, et al. (2001) Down syndrome congenital heart deases: a narrawed region and a candidate gene. Genet Med 3: 91-101.
- Grech V, Gatt M (1999) Syndromes and malformations associated with congenital heart disease in a population-basedstudy. Int J Cardiol 68: 151-156.
- Freeman SB, Taft LF, Dooley KJ, Allran K, Sherman SL, et al. (1998) Population-based study of congenital heart defects in Down sundrome. Am Med Genet 80: 213-217.
- Stoll C, Alembik Y, Dott B, Roth M (1990) Epidemiology of Down syndrome in 118, 265 consecutive births. Am J Med Genet Suppl 7: 79-83.
- Fallot A (1888) Contribution to the pathological disease of the blue disease (cardiac cyanosis). Medical Marseille 25: 77-403.
- Bonnet D (2001) Treatment of chronic heart failure in children. Pediatr Arch 8: 1379-1382.
- Ali SK (2009) Cardiac abnormalities of sudanese patients with down’s syndrome and their short-term outcome. Cardiovasc J Afr 20: 112-115.
- Abbag FI (2006) Congenital heart disease and other major anomalies in patients with Down’s syndrome. Saudi Md J 27: 219-222.
- Tulloh RM, Tansey SP, Parashar K, De Giovanni JV, Wright JG, et al. (1994) Echocardiographic screening in neonates undergoing surgery for selected gastro-intestinal malformations. Arch Dis Child Fetal Neonatal 70: F206-F208.
- Cohen L, Hazelzet T, Zoghbi J, Lecompte Y (2009) Surveillance and treatment of large children and operated adults of tetralogy of fallot. J Practical Cardiol.
- Legloan L, Abbey S (2009) Follow-up of patients with tetralogy of Fallot in practice. J Practical Cardiol.

