Keywords
Workload; Wellbeing; Nurses; Intensive care unit; Job demand resource model; Saudi arabia
Introduction
According to the World Health Organisation (WHO), a healthy workplace environment is essential, where workers and managers collaborate for continuous quality improvement processes, to protect and promote the health, safety and well-being of all employees [1-19]. The shortage of specialized ICU nurses because of the above factors may, therefore, impact on their ability to stay focused to provide quality and safe nursing care and can contribute to their well-being thus affecting their ability to be productive. As a result, working in ICU's might be perceived as stressful and demanding emotionally with possible poor health outcomes for nurses' well-being [13].
Nurses’ workload is increased by shortage of nurses and increasingly, they have to play more versatile roles which increases the work demands [15]. Practical methods of studying workload among ICU nurses were reviewed and analyzed by Kwiecie?et al [14], who concluded that the measurement of workload was an important focus among healthcare workers. Workload represents an important context for studying the well-being of nurses because of different factors that impact on their mental health, optimal social functioning and performance of work tasks such as patient care delivery, which clearly demands a significant amount of employees’ time and effort. Findings from literature searches revealed a generalized focus on challenges faced by ICU nurses for example, stress, and burnout and job dissatisfaction. These findings then became a catalyst for this study, whereby the researcher aimed to develop a comprehensive healthcare managerial framework that explicated the manner in which workload factors influenced nurses’ well-being in the critical areas in a Saudi Arabian Hospital.
There is an increase in demand for critical care services in Kingdom of Saudi Arabia and globally, this demand is attributable to the increasing population age, longer survival of previously incurable diseases, and advanced surgical procedure that makes post-operative intensive care admission mandatory. Most nurses working within the Saudi Arabian healthcare system come from other countries and should they terminate their contracts for whatever reason, the Saudi Arabian healthcare system and public hospitals will be faced with a crisis due to loss of human resources. Therefore, job satisfaction and well-being are important for the Saudi Arabian healthcare system to retain workforce from outside the country. Researchers have found that there are many workload variables, such as work environment, age, job demands, level of skills and patient and organisation expectations that can influence nursing well-being [10]. Despites the identification of workload factors or stressors on ICU nurses, during literature search, the Saudi Arabian ICU nurse perspective of such stressors and its influence on their wellbeing remains an under researched area.
Purpose and Problem Statement
Our purpose was to explore various workload factors experienced by the ICU nurses with the aim of developing a comprehensive health care managerial framework that explicated the manner in which workload factors influenced the ICU nurses wellbeing.
The healthcare system and the health infrastructure in Saudi Arabia are improving and developing gradually. Nevertheless, the shortage of nurses and the increase demand in the numbers of Saudi Arabian hospitals for national nurses have become critical issues for health policymakers. There is an increase in demand for critical care services in Kingdom of Saudi Arabia and globally, this demand is attributable to the increasing population age, longer survival of previously incurable diseases, and advanced surgical procedure that makes post-operative intensive care admission mandatory. Most nurses working within the Saudi Arabian healthcare system come from other countries and should they terminate their contracts for whatever reason, the Saudi Arabian healthcare system and public hospitals will be faced with a crisis due to loss of human resources. Therefore, job satisfaction and well-being are important for the Saudi Arabian healthcare system to retain workforce from outside the country. Researchers have found that there are many workload variables, such as work environment, age, job demands, level of skills and patient and organisation expectations that can influence nursing well-being [10]. While there is a plethora ofsearched literature on patient safety, medication errors, job satisfaction, factors contributing to intention to leave, burnout and workplace stressors there is little information on the impact of workload factors on nurses' well-being in ICUs from a nursing perspective in Saudi Arabia. Therefore, a greater understanding of nurses’ experiences will not only provide a baseline from which to work, but it will help raise awareness of ICU's nurses’ well-being related to their workload.
Significance
ICU nurses play versatile roles and their workload extends beyond the care of the patient with additional team and organisational responsibilities. Their well-being can be conceptualized as a spectrum, with flourishing, happiness and high well-being at one end, and elevated depression, anxiety and low well-being at the other. Human factors are important contributors and play an important role for staff well-being. Research on these associations is imperative and relevant now more than ever due to increased pressures on healthcare service budgets causing growing concerns around staff working conditions, morale and well-being.In Saudi Arabia, there are no studies focusing on workload and well-being among nurses in an ICU environment. Most of the studies are related to workload and patient safety. Work pressures are evident in health systems where there is growing concern over a nursing shortage in relation to the country's disease profile, population increases, chronic disease growth and increased life expectancies. It was important to explore the experiences of nurses working in an ICU environment in a Saudi Arabian Hospital in Southern Region of Saudi Arabia. It is envisaged that further recommendations from this study, with the early identification of the various workload factors, with possible early detection and intervention strategies may assist in preventing factors leading to staff dissatisfaction and thereby assist in promoting staff retention.
Literature Review
The literature review was an interpretation and the study of literature, which followed a topic of enquiry and attempted to identify and track down all the available literature on the topic by following a clear comprehensive methodology from an international perspective. The nursing needs of Saudi Arabia far exceed the supply of Saudi nurses. Despite continued efforts to increase the number of Saudi nurses by 2010, expatriate nurses still constituted 74% of the total nursing workforce in Saudi Arabia. In Saudi Arabia, nursing is a less desirable career choice for Saudi nationals in comparison to other professions. According to Abu-Zinadah [3], because of the nursing shortage, Saudi Arabia needs 25 years to train ICU Saudi nurses to cover 30% of the nursing labour requirements.
An increase in nurses’ workloads has implications for nurses, patients and the organisations. The work environment of nurses has changed significantly in the past few years due to factors, such as health reforms, hospital renovations with structural changes, the shortage of nurses in the face ofrapid technological advances, and patients' expectationsof high-quality services with best and safe outcomes [14-16]. However, recent reports and studies indicate a decrease in nurses' health benefits during patients' treatment, because of their high workload. Therefore, nurses' work pressures and workload are not only determined by a functional framework, but also by many cognitive factors which affect them, indicating the complexity of their tasks state that nurses' workload factors were not only determined through a specific package or structure of guidance but by many other factors which include cognitive factors and the complexity of nurses' work environments which are significant in the accurate estimation of nurses' workload experiences. Work pressures were considered as a critical function of time which was influenced by factors such as the level of complexity, and the number of services provided. The factors relating to process and activity had a significant effect on nurses’ workload. The factors of the process components include the mismatch between the capacity of the wards or the units and the number of patients admitted, and the factors of the activity components include assisting and mentoring the students and newly recruited staff.
The main determinant of nursing workload, at the patient-level, is the clinical situation of a patient. The situation-level includes factors, such as physical working environment, lack of appropriate and adequate provision of resources and facilities, diversity of family needs, and ineffective communications between members of a multidisciplinary team, which can increase the situational workload.
The multi-level human factor framework for workload (Figure 1) illustrates the outcomes of the demand resource factors from unit-level, job-level and task-level. Quality of care and quality of working life in health care are off-cited targets for improvement (Institute of Medicine 2005: 90). Substantive improvements in both can be achieved by understanding health care work system in conjunction with human factors design and redesign. The human factor framework indicates that excessive nursing workload is one of the contributors to quality of care and working life problems that has been internationally recognised as needing further study and remediation. While the nursing workload presents a challenge for the workforce sectors globally, not much attention has been given to the determining factors and the outcomes. It is critical to understanding these factors to help nursing managers and leaders to provide suitable working environments and to manage the adverse outcomes of the nursing workload.
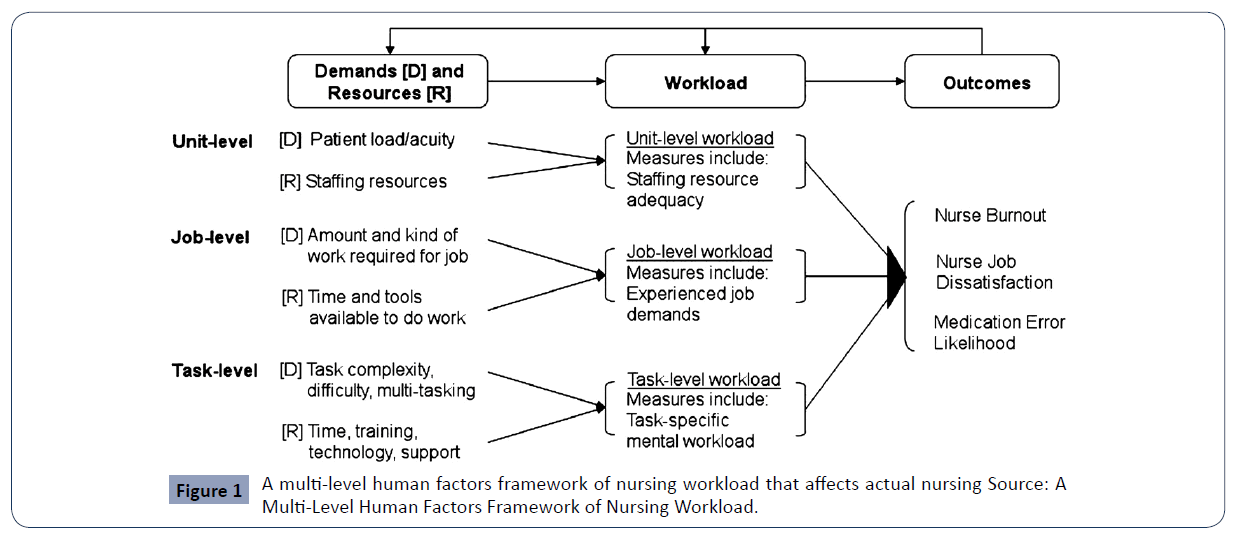
Figure 1 A multi-level human factors framework of nursing workload that affects actual nursing Source: A Multi-Level Human Factors Framework of Nursing Workload.
According to this multi-level human factor framework, the level of workload depends on the type of nursing job or speciality (ICU nurse versus operating room nurse). However, workload is a complex, multi-dimensional construct, and there are several contextual factors in a nursing work environment, such as performance obstacles and facilitators, other than job title that may affect nursing.
It has also been noted, that although high job demands are accompanied with the demand for enough job resources, the outcome can be a positive one resulting in increased staff morale, motivated staff and increased job satisfaction.
Methodology
The present study adopted a mixed method convergent parallel design [11], which included separate analysis of the quantitative and the qualitative data, which were collected separately. This paper will concentrate only on the qualitative data findings.
Target population
In this study, the target population were ICU nurses (N=200) working in the ICUs at the Saudi Arabian hospital keeping in mind that the sample size of a qualitative study cannot be predetermined and it was dependant on the availability of nurses who met the inclusion criteria and gave voluntary consent.
Sampling
A purposive, non-probability sampling strategy method was used to recruit nurses to participate in the semi structured interviews for the qualitative phase of the study n=20. At total of 20 interviews were conducted over a period of two weeks. The researcher invited the nurses (n=20) from the different ICUs in the hospital to participate. Nurses who met the criteria were provided with information on the research and invited to participate.
Data Collection
Now from here just concentrate on the qualitative aspects
Two data collection strategies that are typically used in mixed method convergent parallel design study research, namely interviews and surveys by use of questionnaires will be used in this study. The aim of using multiple strategies in this study was to increase the validity of its findings and ensure a thorough understanding of concepts related to workload factors and its influence of nurses’ well-being in the ICU environment.
Data collection was conducted in two phases. Phase 1 began with the qualitative strand of the study and sought to assess how the ICU nurses perceived workload factors and its influence on their well-being within the critical care environment. It also aimed to develop a comprehensive managerial framework that explicates the workload factors and its influence on ICU nurses. In Phase 2, the quantitative strand of the study was undertaken and explored the experiences of the ICU nurses staff that were directly involved on the ward level with clinical patient care. The researcher aimed to conduct all phases of the research study on her own in separate phases
Data analysis
The study consisted of two data sets: qualitative data and quantitative data, both of which needed to be analysed and interpreted in order to conclude study findings and to develop a comprehensive managerial framework that will explicate workload and its well-being among ICU nurses in a Saudi Arabian hospital during the final stage of the study. The two sets of results were then compared and interpreted in the data analysis The quantitative data was analysed using latest version of SPSS and qualitative data was analysed using Tesch’s method of data analysis.
Ethical considerations
Ethical clearance was obtained from the University Institutional Research Ethics Committee and a written consent was obtained from all participants who made an informed, voluntary decision to participate.
Trustworthiness and research rigour
The researcher ensured the rigour for both qualitative and quantitative methodologies as the two strands were both incorporated in the mixed method design. The most important steps in mixed methods studies is when the results from the study’s qualitative and quantitative strands are incorporated into a coherent conceptual framework that provides an effective answer to the research question.
Trustworthiness qualitative data
The study’s qualitative nature allowed Lincoln and Gubas strategy (creditbity, transferability, dependability and conformability) to be applied to enhancing trustworthiness, Creditibity in this study was achieved by accurately describing the study’s parameter such a whom, where and when Transferability was promoted by ensuring that the research process was accurately described to all participants. The techniques to ensure trustworthiness followed Lincoln and Guba’s recommendations using the criteria of credibility, dependability, conformability, and generalizability.
Research Findings
Qualitative findings
The average age of the respondents ranged from 21 years and above 50 with the majority of the respondents n=107 (53.5%) were within age 31-40. The majority of the respondents were mature adults ranging from 31 years to above 50 years. The modal tenure related to service to the organisation was between 3-7 years. Majority of the respondents were loyal to the organisation and had spent more than 5 years within this organisation. This was interpreted as commitment and loyalty to the organisation and also good working environment related to length of stay greater than 5 years. The predominant nationalities were Indians within the ICUs n=141 (70.5%) of the sample and Filipino n=44 (22.0%) of the sample. The results can be interpreted as the majority of staff in the critical care areas are of Indian Nationality, in comparison to Saudi ICU nurses, whereby the percentage is only 2.0%. This is of high concern for the future of Saudi Arabia with the Saudisation programme and the country 2030 vision to reduce the employment of foreign nurses. The analysis showed that a large percentage of respondents experienced various emotional or physical impact on their health at different levels from work related issues. Seven Themes and several sub themes emerged during the semi structure interviews with ICU nurses. Themes and Sub Themes are presented in Table 1.
| Major themes |
Sub-themes |
| Theme 1: Shift work and its impact on work life. |
1.1 Psychological concerns of shift work. |
| 1.2 Physical concerns of shift work. |
| 1.3 Workplace productivity related to shift work. |
| 1.4 Moral distress issues resulting from shift work. |
| 1.5 Occupational exposure during shift allocation. |
| Theme 2: Human resource concerns. |
2.1 Nurse-patient ratios during work allocation. |
| 2.2 Patient allocation in the ICU work environment. |
| 2.3 Shortage of skilled labour ICU work environment. |
| 2.4 Shortage of medical and surgical supplies in the ICU work environment. |
| 2.5 Budgetary constraints and its effect on ICU functioning. |
| Theme 3: Cultural barriers to communication. |
3.1 Language barriers and its effect on communication. |
| 3.2 Multicultural diversity of staff and its impact on communication. |
| 3.3 Support systems to assist with staff communication challenges. |
| Theme 4: Factors influencing staff turnover in the ICUs. |
4.1 Staff attrition and its influence on staff turnover. |
| 4.2 Staff absenteeism and its impact on staff turnover. |
| 4.3 Staff job satisfaction and its influence on staff turnover. |
| 4.4 Staff Retention and its impact on staff turnover. |
| Theme 5: Group cohesion in the workplace. |
5.1 Decision making and team building in the workplace. |
| 5.2 Psychosocial barriers to teamwork in the workplace. |
| 5.3 Human respect and value systems in the work place. |
| 5.4 Team work and teambuilding in the workplace. |
| Theme 6: Emotional exhaustion factors in the workplace. |
6.1 Sleep deprivation and its influence on emotional exhaustion. |
| 6.2 Fatigue and distress and their influence on emotional exhaustion. |
| 6.3 Work life balance and its influence on emotional exhaustion. |
| Theme 7: Safety and security concerns in the workplace. |
7.1 Fear of working environment and its influence on safety and security. |
| 7.2 Physical and verbal abuse of staff and their influence on employee safety. |
| 7.3 Lack of respect and human dignity and its influence on safety and security. |
Table 1 Summary of Themes and sub-themes that emerged from the Interviews.
When participants were asked to rate their quality of life in relation to psychological and emotional well-being after 12 hour shifts, some of the participants expressed their unconscious prejudices towards the current scheduling process. They overtly expressed their concerns regarding the scheduling of shifts with mixture in a week day and night as this added to their imbalance in social life and also the physiological coping skills with only one day off then another 12 hours to work. Participants strongly verbalised that long working hours contributed to their occupational exposure, as they had to stand on their feet for long hours, resulting in physical and emotional exhaustion.
One participant responded as follows: “Quality of life, can be rated one as the least and ten as the maximum and after twelve hours shift I will rate it to 5. Five because you will be exhausted after the long working hours and this affects you, physically and emotionally”.
Human resource concerns
Participants expressed great concerns regarding staffing and other resources such as supplies that was creating a barrier between the job and the outcomes related to safe patient care. Many of the participants expressed the age factor and years of experience which was a contributing to job strain and inability to cope with workload. The other factor that contributed to human resources were shortage of staff and lack of skilled nurses. Many skilled nurses were beginning to retire or leave the profession which is resulting in a problem of supply meeting the demand. Some of participants expressed that the management needs to focus factors to employ more skilled and experienced staff to overcome work related stress. Participants were very expressive to maintain an appropriate mix between the different types of health promoters and caregivers to ensure the system's success.
This was noted in one of the excerpt: “Some consequences during the working shift is related to incomplete tasks due to not enough time to complete the clinical tasks. We forget something during the day and it will affect us that much with the patients. Sometimes because of the stress of the job and nurse patient ratio for example instead of 1:1 we take 3 patients and at timesthe increase in the work tasks you tend to forget some of these care processes to be delivered to the patient”.
Cultural barriers to communication
The Kingdom of Saudi Arabia is a highly conservative nation that adheres to the code of morality based on Islamic traditions. This code is imposed not only on the native Saudi population, but on foreigners residing in the Kingdom as well. Nurses who came from other countries are non-Arabic speaking resulting in difficulties in communication between nurses and patients as well as between nurses and medical staff from other nationalities. In Saudi Arabia, international nurses’ language may differ from that of the local Saudi patients for which they care, jeopardising their ability to communicate effectively. The possibility of passing the wrong message increases when the nurse and the patient speak different languages.
One of the participants responded as follow: Because of the different nationalities and the various spoken languages some staff experience difficulty in the communication. Some are very good with the Arabic language and is able to converse effectively between some of them but the alternate is challenging for others where they’re not able to communicate on the same level and that can be, in terms of patient care related issues it can have a negative impact. Patients and families cannot speak English and this creates that language barrier” (Participant 2, Female, ICU).
Factors influencing staff turnover in the ICUs
Majority of the participants during the interview expressed their feeling of being over worked and shortage of staff which contributed to their emotional exhaustion and wanted to leave the organisation. Some expressed their dissatisfaction with the shortage of stock and the general environment and predominantly the cultural barriers that impacted on their work due to lack of respect from the patients and families. The most common factor that was causing the intention to leave was the communication elements and poor working relationship with the doctors within the ICU environment. Doctors were seen to be disrespectful and unappreciative towards the nurses and they adopted a blame culture.
This was noted in the following excerpts: “Due to high apathy and high workload we've become more emotionally and physically drained plus the fact that we are away from our family and we have no one to talk to when we arrive in our accommodations. No job satisfaction due to all the challenges such as shortage of staff low salary no increases and no security for us a foreigners and no respect. Yes we want good working conditions and will stay but no respect from patients, doctors and management then we will leave due to no job satisfaction”.
Group cohesion in the workplace
Majorityof the participants expressed their views about lack of team work among their colleagues, doctors and the multidisciplinary teams. In their opinion they believed that they spend majority of their time performing non nursing tasks of other areas such as physiotherapy and following up on laboratory results and this took them away from the patients’ bed side. The increase in the work load and the communication also contributed to lack of team work within the various ICUs. Nurses had no time to reflect and discuss their challenges as a team due to high work demands. Some of the participants expressed some strategies to improve the retention rates of nurses in the ICU and recommended that management need to focus on building a cohesive workforce by utilising the strengths and skill sets that characterise different generations of nurses, and should create working conditions in which nurses across all generations feel supported and safe within the organisation.
This was noted in the following verbatim responses: “Conflict in the work place, especially with our colleagues. And you know, trust issues are a very worrying issue in the unit. You don’t trust anybody because you feel that you know, they are not there to protect you, you are always on your own, especially when things happen at the bedside, that you are the one that gets blamed. So, you can't trust the next person. And also, obviously fear. Fear of our environment”.
Emotional exhaustion factors in the workplace
Health care institutions, and patients, in particular will benefit the most from a healthy and rested nurse because her efficiency and productivity will be increased, the number of work-related mistakes is reduced, sick leaves are rarer and shorter, and burnout does not occur. By focusing and introducing well-being strategies, we would not only reduce the emotional exhaustion factors among nurses but would also significantly raise the quality of their work. Some of the participants expressed their concerns about being exhausted after long shifts. Some of the participants expressed that in stressful situations they had trouble concentrating and felt unmotivated to work, and entered into conflicts with patients and co-workers. Their emotional concerns were related to workplace cultural factors, language barriers and errors in judgement.
One of the participants responded as follows: “For the 12-hour shifts, it is exhausting that even if we are going home after the shift we will not be concentrating on our self. We will not be resting or sleeping, we will not eat enough. The routine of sleeping, going to duty, sleeping, going to duty, becomes monotonous.It’s like a pattern…and our families would be affected also. We will not be having time to be with them because we too tired after long shifts”.
Safety and security concerns in the workplace
Majority of the participants expressed security issues during the interviews. They did not feel safe in this environment and expressed their disaffection about the security in the units. Some of the participants strongly verbalised that management should look into this factor as this was their biggest fear being foreigners and fear was unexplained. Nurses in the present work perceived that the shortage of nursing staff and security personnel were the main causes of violence against them. From the interviews, it was clear that violence against nurses is a serious public health problem and an improvement in the security provided in hospitals may help to alleviate this issue. It was also recommended by the participants that the community awareness of this problem needs to be improved and some system to be in place to change the attitude of patients and the community and management to protect the nurses.
This was evident in the following responses: “I would say, we should first and foremost secure the safety of our staff in the organisation. You know, improve safety, get more security and protect our nurses from the violence in the workplace. Also, when such incidents happen to our staff, that management needs to deal with that immediately and effectively, not that the staff will feel that you know, they are being victimised because no action is being taken when a patient or a relative attacks them”.
Conclusion
Healthcare organisation across the globe is challenged to achieve nurse workforce stability, safety, and well-being. Environmental characteristics examined in this study have ranged from staffing and resource adequacy as well as the support of unit level and organisation wide managerial support. A variety of job related experiences were linked with high turnover as well as impaired well-being factors related to job demand resources. In this study, workload played an important mediating role between the extent of well-being and emotional exhaustion among ICU nurses. The model of job demand resource was grounded in theoretical assumptions and previous study findings, and appears to explain nurse job outcomes and experiences of well-being. On the whole, this study revealed that employee well-being had a strong influence by the various workload factors. This study sets out the key messages for health care managers to empower and to meet the needs of ICU nurse related to health and well-being The interventional strategy will build on good practice and evidence drawn from a range of professional and partners including, Allied Health Professionals, doctors, social care, practice nurses and managers. Executive and middle management providers will be at different points of development and can use the strategy to benchmark their current position and to drive improvements from the findings of the study.
35560
References
- Abo-Znadh SH (1999) An exploration of selected staff and job characteristics, and their relationship to quality of work life, among staff nurses in medical/surgical units in two tertiary care hospitals in Saudi Arabia. George Mason University, Fairfax, Va.
- Abdi H, Shahbazi L (2001) Correlation between occupational stress in nurses at intensive care unit with job burnout. J Shahid Sadoughi University of Med Sci 9: 58-63.
- Abu-Zinadah S (2006) Nursing situation in Saudi Arabia. Riyadh: Saudi Nursing Board, Saudi Commission for Health Specialities.
- Adair JG, Vohra N (2003) The explosion of knowledge, references, and citations: Psychology’s unique response to a crisis. American Psychologist 58: 15-23.
- Aiken LH, Sochalski J, Anderson GF (1996) Downsizing the hospital nursing workforce. Health Affairs 15: 88-92.
- Aiken LH, Clarke SP, Sloane DM, Sochalski JA, Busse R, et al. (2001) Nurses’ reports on hospital care in five countries. Health Affairs 20: 43-53.
- Bakker AB, Demerouti E, Schaufeli E, Sanz-Vegell AI (2014) Burnout and work engagement: The job demand resource approach. Annual Revision of Organisational Psychology and Organisational Behaviour 1: 389-411.
- Bakker AB, van Veldhoven M, Xanthopoulou D (2010) Beyond the demand-control model: Thriving on High Job Demands and Resources. J Personnel Psychology 9: 3-16.
- Baldin A, Bray K, Gibson V, Goodman S, Ledger U (2010) Standards for nurse staffing in critical care. British Association of Critical Care Nurses 15: 109-111.
- Borkowski N (2011) Organisational behaviour in health care (2nd edn). London: Jones and Bartlett Publisher International.
- Creswell JW, Plano Clark VL (2011) Designing and conducting mixed methods research (2nd edn). London: Sage.
- Greene JC, Caracelli VJ, Graham WF (1989) Toward a conceptual framework for mixed-method evaluation designs. Educational Evaluation and Policy Analysis 11: 225.
- Hsu HY, Chen SH, Yu HY, Lou JH (2010) Job stress, achievement motivation and occupational burnout among male nurses. J Adv Nurs 66: 1592-1160.
- Kwiecień K, Wujtewicz M, Mędrzycka-Dąbrowska W (2012) Selected methods of measuring workload among intensive care nursing staff. Int J Occup Med Environ Health 25: 209-217.
- Stordeur S, D’hoore W, Vandenberghe C (2010) Leadership, organizational stress, and emotional exhaustion among hospital nursing staff. J Adv Nurs 35: 533-542.
- World Health Organization (2015) Analytical summary. Health workforce. African Health Observatory.

