Keywords
Neurological rehabilitation; Schema therapy; Executive functions; Chronic depression.
Introduction
Everyone may have a feeling of depression at some time in his/her life, and usually relates it to a specific event. Two types of events are particularly important in causing depression: loss and failure. Experiences, such as job loss or the death of close relatives would be the beginning of a period of grief, and constant repeating of some negative thoughts. Also, failures such as failing a test or failure to convince a person of interest to get married can also cause frustration and negative thoughts and feelings (such as pessimism and self-doubt).
Most people who have negative feelings can stop them in a matter of days or weeks and return to their normal lives ;but for some people, symptoms of depression persist for a long time and influence all aspects of their lives.
Also, they have negative impacts on emotional, behavioral, cognitive, and physical aspects and may lead to clinical depression. Chronic depression causes people not to be able to do ordinary things in their daily lives as well. Sometimes depression happens without occurring negative events, such as loss or failure and sometimes it takes much more time than what is expected.
In depression, emotional, motivational, cognitive, behavioral and physiological symptoms are seen that include sadness, lack of energy , oversleeping, appetite and intense cravings for carbohydrates, overeating and weight gain. According to DSM-5, permanent depression disorder is actually a combination of major chronic depressive disorder and dysthymic disorder. 12-month prevalence rate of depression in America is about 0.5% for permanent depression disorder and to 1.5% for chronic depression disorder.
Among the variables vulnerable to chronic depression disorder, there are executive functions. Executive functions include behavior complex planning and problem-solving actions involved in patients daily life. The activities that require executive functions, include meeting timetables, understanding medical information, riding a motorcycle, the appropriate use of medicines, cooking, wearing clothes and doing housework. Executive functions are cognitive processes that coordinate the complex activities. Depression can have a prominent role in executive functions and in this relation, "numbness" is expected to be associated specifically with executive dysfunction since these symptoms are more related to depression (For example, lack of interest in activities and numbness).
In addition, it is assumed that depression symptoms are partly due to the relationship between PTSD and performance. Patients with chronic depression show cognitive-functional defects similar to those seen in patients with major depression.
Verbal remembering scores in both groups of patients, negatively are linked with depression rate measured by Hamilton Depression Scale, but positively are linked with scales composed of executive functions measured by Wisconsin Card Sorting Test (WCST).
In several studies , different reasons have been considered for executive function deficits in depressed patients, including denderitic deterioration, bad chemical regulation in the prefrontal cortex and hippocampus tissue , lesions in frontal white and gray tissue, lack of dopamine (DA) in striatum and extra striatal region such as the prefrontal cortex and anatomical changes in frontal and temporal parts [1].
Researches discovered deficiencies of executive functions in depressed patients. Ravankilde, Videbech, Clemmensen, Egander, Rassusen, Rosenberg found that patients with depressive disorders have difficulty in the regulation of executive functions in daily life. Also Young et al. [2] reported on executive inactiveness in some behaviors such as attention, memory and distraction. In this study also evidences have been reported on depressed patients inability in determining appropriate responses to environmental and memory functions.
What the findings of Ajilchi, Ahadi, Nejati and Delavar showed was that executive functions in depressed patients significantly are more than ordinary people.
A current treatment that is used widely for depression is schema therapy. One of the main goals of schema therapy is establishing healthy interaction dealing with internal flexible, positive, and creative aspects. The combination of cognitive and experimental techniques (a two-side communication) can be set up between part of person having schemas and the healthy section which rejects incompatible beliefs.
Since healthy sound can be unfamiliar to patient, so a common text and document can be created. Initially, the patient acknowledges a schema side. Then the therapist acknowledges the healthy side and then vice versa. The patient is encouraged to engage in the two-side dialogue, think about them and then can accept one side and denies the other side. These needs are done recurrently, so the patient can be fully integrated into the conscious awareness of them in his view to the world [3].
Since the most schemas involves interpersonal relationships, they can be tested in the context of the treatment. There can be good opportunities for this issue when the patient misinterprets what the therapist says or may be shows emotional agitation. Nonverbal symptoms can be another important source of information. When the therapist and the patient are involved to clarify the cognitions and emotions and relate them to specific schemas, truth evaluation can occur [3].
Research results from Imel et al., Cuijpers et al. and Schramm proved the effectiveness of this therapy to improve depressed patients cognitive distortions, irrational beliefs and executive functions.
While integrating schema therapy, we have also benefited neurological rehabilitation. Neuro-psychotherapy is a method of treatment based on recent advances in the field of neuroscience, neurological and psychological rehabilitation and psychotherapeutic techniques. This method signifies the proximity and integration between theoretical and clinical knowledge as well. The pioneer of holistic neurological rehabilitation was named Niilo Maki (1902-1968) and he benefited neurological rehabilitation to treat injured war soldiers. Klaus argues that in neuro-psychotherapy there is more emphasis on principles of neuroscience in psychotherapy. In this regard, he suggested that psychotherapists should have knowledge on the fundamental issues in nerve system involved in mental disorders. He considers nerves flexibility as a positive point in psychotherapy, and says: intensive use of certain areas in brain or stimulating there and sometimes neutralizing stimulations can lead to structural changes in the brain. Indeed the purpose of neuro-psychotherapy is inspiring changes in brain and by focusing on the experiences happened in life and these experiences gain meaning referring brain structures.
Vynksy & Carney in a study have reported the independent effectiveness of this therapy to improve executive functions and treating depression in patients with chronic depression. The results of studies of Pinto & Gouveia indicated the effectiveness of this type of therapy in reducing anxiety, tension, anxiety sensitivity and improving symptoms of depression and executive functions in depressed patients.
This study is seeking to answer the question as “whether schema therapy integrated with neurological rehabilitation can affect the executive functions in patients with chronic depression?”
Method
The research method used in this study is a pilot test with single case and multiple baselines. In this pilot project, test variables are just applied for one person, behavior or situation (after the baseline). This can also be used for one person or a small group.
Community, samples and sampling
The research community includes the patients with chronic depression who attended the counseling and psychotherapy department in Teachers Specialized Clinic, situated in 13th District. The samples are from men and women who had chronic depression and were referred to this center in Tehran, in 1393. They were selected by "convenience sampling". Finally, after referring patients based on entering criteria to the study and doing the Structured Clinical Interview to diagnose (SCID) I axis disorder, the patients were checked out relating exiting criteria by psychiatrists.
After selecting the 6 subjects, each time two participants entered the baseline stage simultaneously into third, eighth and twelfth sessions. The method was in a way that every 6 subjects participated in baseline stage and subsequently entered the stage integrated with neurological rehabilitation methods. The following tools were used to collect data in this study:
Structured clinical interview for axis I disorders (SCID-I)
The interview is a flexible tool developed by First et al. Sharifi et al. translated the interview into Persian and conducted it on 299 subjects. Diagnostic agreement for most specific and overall diagnosis was average or effective (Kappa above 60%). General agreement (total current diagnose Kappa was 52%) and an overall lifetime diagnose was 55% obtained was also satisfactory.
Beck depression inventory (BDI-II)
Beck Depression Inventory was proposed to measure depression. This version is more consistent with DSM-IV compared to the first edition, as the BDI, BDI-II have 21 questions (from 0 to 3) and cover all aspects of depression based on cognitive theory. The overall score is variable between 0 and 63, the scores from zero to 13 show minor depression or no depression, 14 to 19 show mild depression, 20 to 28 moderate depression and 29 to 63 indicate severe depression. Beck, Steer and Brown studies showed that the questionnaire has high internal consistency. Other studies reported internal consistency of this scale (Cronbach's alpha=0.93) and retested reliability of (r=0.93).
Wisconsin card sorting test
This test has been used to evaluate the executive functions of depressed patients. In this test, abstraction potentials and the ability to change cognitive strategies in response to changing environmental feedbacks are being assessed. Herewith, the person requires planning, organized searching and the ability to use environmental feedbacks to change cognitions. Based on Goldberg and Weinberger, the test is one of the most sensitive tests relating prefrontal and posteriorlateral cortex. Anderson, Damasio, Jones, Tranel also consider this test as a scale to measure damages to frontal cortex.
Lezak assumes 0.86% validity for this test to assess cognitive deficits due to brain damages. The reliability of the test, according to Aspirin & Strauss, has been reported as 0.83. Naderi considers 0.85% of the test reliability for Iranian population.
Method
In this study, after proving the diagnose of chronic depression by the therapist, patients are being practiced under the treating intervention which is schema therapy integrated with neurological rehabilitation. It is done after asking for the consent of patients and explaining the project to them.
Therapy sessions are held for 15 weekly sessions of 60 minutes. At the beginning of the study, all the patients had to complete their research tools. Then the schema therapy for chronic depression was practiced and followed for almost 2 months to determine the stability of the therapeutic effects. The criteria for precluding the patients from treatment process was two successive absence from the sessions. Eligible research subjects were selected from the men and women who attended the clinic (Tehran East Branch of Teachers Clinic). Then the participants were under the practice of interventions. After the third, eighth, twelfth sessions and also at the end of the therapy sessions, all were tested and there was a final two-month follow up.
In this study, data analysis is done on the basis of charts review and impact factor methods. The formula used to calculate the percentage of recovery is:
MPI=[(Baseline Mean – Treatment Phase Mean) / Baseline Mean] × 100
Recovery Percentage Formula is a method to measure progress in reducing the problems that clients are targeted. This formula was used by Schwars & Blanchard. In this formula, we subtract the pretest score from the score in posttest then divide the result by the pretest score. If the answer shows at least 50 percent improvement in terms of results can be considered clinically significant (according to Ogles, et al.).
The results show that the subjects scores have improved after the treatment (Table 1). Total data proves that treatment based on schema therapy integrated with neurological rehabilitation methods has reduced subjects’ scores. Based on the table, scores on each of the six participants in the Wisconsin Card relating retardation errors are reduced during sessions which signifies the efficacy of schema therapy integrated with neurological rehabilitation in reducing retardation errors. The recovery index for each of the six participants in Wisconsin Card scale regarding errors are in turns (56.75, 64.06, 68.75, 56.25, 60.01, 57.14).
| Subjects |
Base line |
3rd session |
8th session |
12th session |
Post treatment |
Intervention average |
Follow up session |
Recovery percentage |
Reduction percentage |
| S1 |
9 |
6 |
5 |
3 |
1 |
3.75 |
1 |
56.75 |
0.14 |
| S2 |
16 |
10 |
7 |
4 |
2 |
5.75 |
2 |
64.06 |
178.26 |
| S3 |
12 |
6 |
4 |
3 |
2 |
3.75 |
1 |
68.75 |
0.22 |
| S4 |
8 |
5 |
4 |
4 |
1 |
3.5 |
1 |
56.25 |
128.57 |
| S5 |
5 |
3 |
2 |
2 |
1 |
2 |
2 |
60.01 |
0.15 |
| S6 |
14 |
12 |
6 |
3 |
1 |
6 |
1 |
57.14 |
133.33 |
Table 1 Subjects scores in Wisconsin Cards referring retardation errors at baseline, in treatment, post- treatment and follow-up process.
Since over 50 percent of the recovery shows the effectiveness of treatment, Therefore, we can conclude the treatment method which uses schema therapy integrated with neurological rehabilitation can be effectiveness (Figure 1).
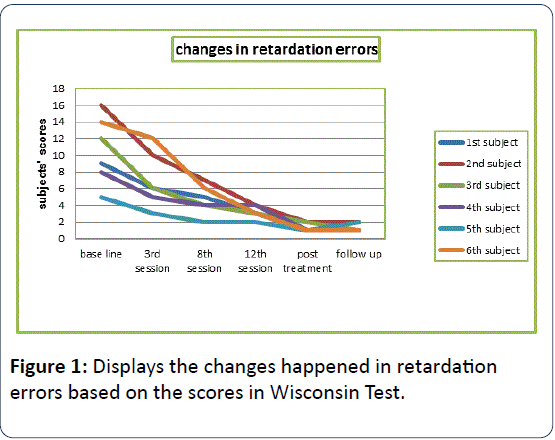
Figure 1: Displays the changes happened in retardation errors based on the scores in Wisconsin Test.
In Table 2, the results show that subjects scores improved in post treatment stage.
| Subjects |
Base line |
3rd session |
8th session |
12th session |
Post treatment |
Intervention average |
Follow up session |
Recovery percentage |
Reduction percentage |
| S1 |
28 |
21 |
14 |
9 |
4 |
12 |
5 |
57.14 |
133.33 |
| S2 |
16 |
11 |
8 |
5 |
3 |
6.75 |
2 |
57.81 |
137.03 |
| S3 |
26 |
18 |
11 |
4 |
2 |
8.75 |
2 |
66.34 |
197.14 |
| S4 |
38 |
33 |
17 |
9 |
3 |
15.5 |
3 |
59.21 |
145.16 |
| S5 |
24 |
18 |
12 |
6 |
4 |
10 |
1 |
58.33 |
0.14 |
| S6 |
26 |
21 |
13 |
5 |
2 |
10.25 |
2 |
60.75 |
153.65 |
Table 2 Test scores in Wisconsin Card relating incorrect responses at baseline, in-treatment, post- treatment, follow-up.
Total data signify that schema therapy treatment integrated with neurological rehabilitation leads to lower scores of subjects. According to the chart, six subjects scores of incorrect answers in Wisconsin Card Scale have lowered during sessions. It is a proof to the effectiveness of the treatment. This can be better understood regarding recovery index of retardation errors which for the six participants are in turn (57.14, 57.81, 66.34, 59.21, 58.33, 57.60). Since over 50 percent recovery signifies the effectiveness of treatment, therefore we can conclude: the treatment through schema therapy integrated with neurological rehabilitation methods have proven effective (Figure 2).
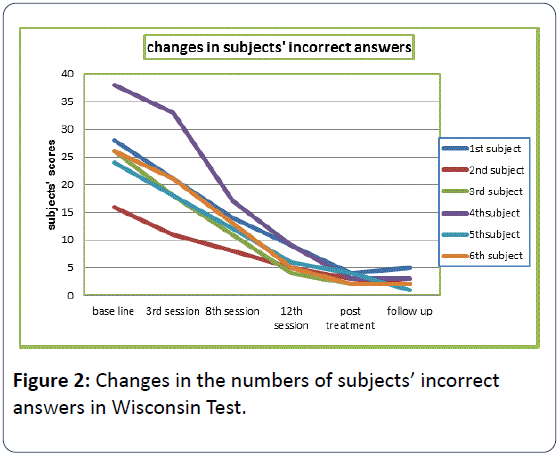
Figure 2: Changes in the numbers of subjects’ incorrect answers in Wisconsin Test.
Conclusion
The aim of this study was to evaluate the effectiveness of schema therapy integrated with neurological rehabilitation on executive functions for patients with chronic depression.
The results showed that this treatment method significantly reduces impaired executive functions in depressed patients. The results are along with the results of Ravnkilde B, et al. and Porter RJ, et al. [4,5]. Based on these findings, we can say patients with chronic depression have cognitive deficits and due to not considering environmental feedbacks and lack of self-regulation, they have more retardation errors comparing normal individuals.
However, depressed people due to lower impairment in cognitive flexibility and working memory can eventually reach a number of levels and apparently have not significant difference comparing normal people. Schema therapy focuses more on understanding the causes of rumination and early maladaptive processes. Because rumination is an executive function activated to reduce cognitive dissonance in response to negative thoughts and feelings of sadness, and indeed is considered a style of coping with depressed mood.
On the other hand, depressed patients have difficulty in identifying abstract or figurative signs and cannot properly assess the rules and assumptions. Schemas cause disorder in memory processes and as a result, deficits in executive function happen. The patient feel deficient in working memory due to negative schemas. The patient thinks: “solving the problems are far from my ability” so his/her memory cannot help to answer correctly to executive tests.
In this regard, Young believes that these schemas are unconditional beliefs and feelings about ourselves happened due to environment relation. These schemas are rigid and inflexible, so resistant to change, and are considered as basic concept of self-assumption towards environment. These misperceptions reduce the executive actions relating environment, and eventually interfere with individual’s attention and memory and threatens executive functions and compatibility [2]. In addition, maladaptive schemas cause the individual lose the ability to manage emotions so would have problem in executive actions and appropriate responses to the environment [6]. So in schema therapy, patients learn how to focus on their practice, in fact all techniques the therapist uses are focused on the patient.
Revealing the causes of schema change, people find that their executive deficiencies are rooted in their thoughts and attitudes already created and can be changed benefiting training. On the other hand, patients can use this technique to trial the hypothesis of schema. Provoking schemas and its relation with current executive deficiencies failure of the current administration represents emotional insights and subsequent schema improvement .In addition, it can promote patients understanding and directs him/her from rational cognition toward emotional experiences.
According to Young, schema therapy is targeted to help unsatisfied emotions in patients to be met. When emotional needs are satisfied during treating process, it would be a proper background for improving the schemas. Early maladaptive schemas basically occur because of unsatisfied emotional needs [2].
One restriction of the present study was its limitation to Tehran. Conclusively, generalizing the results calls for some caution. Also, subjects are not homogenous in terms of variables such as socio-economic status, marital status and occupation. So, it is proposed the schema therapy integrated with neurological rehabilitation be studied on broader groups of patients. It is also suggested that the effectiveness of schema therapy integrated with neurological rehabilitation be examined through group plans within controlling.
9884
References
- Fossati P, Amar G, Raoux N, Ergis AM, Allilaire JF (1999) Executive functioning and verbal memory in young patients with unipolar depression and schizophrenia. Psychiatry Res 89: 171-187.
- John JC, Mark B, Tracy P (2008) Exploring the relationships among early maladaptive schemas, psychological mindedness and self — reported college maladaptive schemas. J PsycholPsychother I: 105-118.
- Martin R, YoungJ (2010) Schema Therapy, In Dobson KS (Eds) Handbook of Cognitive Behavioral Therapies, Guilford press, London, United Kingdom. 317-346.
- Porter RJ, Gallagher P, Thompson JM, Young AH (2003) Neurocognitive impairment in drug-free patients with major depressive disorder. Br J Psychiatry 182: 214-220.
- Ravnkilde B, Videbech P, Clemmensen K, Egander A, Rasmussen NA, et al. (2002) Cognitive deficits in major depression. Scand J Psychol 43: 239-251.
- Young JE, Klosko JS, Weishaar ME (2003) Schema Therapy: A practitioners Guide. The Guilford press, New York, United States.

