Keywords
Neurological rehabilitation; Schema therapy; Cognitive schemas; Chronic depression
Introduction
Chronic depression is a common psychological disease with heavy economic burden and stable disorder in patients. Depression rates of 6%-20% is the most important public health issue.
Researchers believe that several factors, including genetic (biological) and environmental (social and psychological) ones are influential on depression.
In many studies done on the epidemiology of mental patients and especially disorders such as depression, there has been a great focus on social determinants of depression. In particular, studies have proven the relationship between depression and social factors such as gender, marital status and social supports.
In addition, economic disparities such as income, jobs and social levels are associated with depression [1].
Also, based on various psychological approaches, including cognitive perspective, cognitive structures are involved in the creation, stability and relapse, or return of depression.
Therefore, the need to an effectiveness new therapy has been felt more than ever. According to DSM-5, permanent depression disorder in fact is a combination of major chronic depressive disorder and dysthymic disorder.
One of the factors which can affect the continue of depression is the early maladaptive schema in patients. The early maladaptive schemas (EMS) are deep overall patterns composed of memories, emotions, cognitions and physical sensations generally formed in childhood or adolescence. They continue during life and fight for their own survival. These Early maladaptive schemas are highly inefficient and dysfunctional relating themselves and others.
Although the patient knows the schema will cause discomfort, but feels comfortable toward it and gets used to it. Early maladaptive schemas push people toward feeling of consistency and compatibility. Schema impact on future experience and it is dependable in terms of the intensity and range of activities in patients’ minds [2].
Young insists on the basic schema dysfunction and says: “The early schemas are the main structure of psychological damage”. These schemas are continual thoughts and beliefs of a person from the world around and are rooted in one's childhood experiences [3]. According to Beck people with more negative schemas are more vulnerable to chronic depression in future. Early maladaptive schemas are core axis I and II in chronic disorders. Researches reveal that early maladaptive schemas can contribute to the continuity of a chronic depressive disorder. Young's study showed that the mechanisms which cause movement in schemas can prevent mental disorders and depression. Also findings from Camara and Calvete offer that early maladaptive schemas create anxiety and depression. The formation of defective schema causes unacceptability, damage to self and being guided by others, that all leads to the symptoms of anxiety and depression.
According to the records of schemas and their role in depression, devising a schema therapy approach integrated with neurological rehabilitation seems necessary. Schema therapy, is an innovative and comprehensive approach which was introduced by Young et al. in 1990. In fact, this approach significantly develops cognitive and behavioral therapies and concepts. This type of treatment is a new system of psychotherapy, especially for patients who suffer chronic diseases, such as severe personality disorders and severe depression. In 1990, Young suggested schema therapy for patients who had not responded to other treatment methods. Young argues that schema therapy is a comprehensive and modern treatment based on cognitive therapy and traditional behavioral-cognitive approaches [3]. Numerous studies found this approach effective in the treatment of depressive disorders and generalized anxiety disorder [4] panic disorder [5], social phobia [6,7] eating disorder [8,9] couples problems [10] drug abuse [11] and hospitalized severe depressions [12]. Also the researches of Imel et al., Cuijpers et al., Schramm [13] indicated the effectiveness of this therapy to improve cognitive distortions, depressed patients irrational beliefs and executive functions.
In holistic theoretical system, neurological rehabilitation intervention is one of the latest interventions of behavioral sciences in this domain and it was codified by Niilo Maki (1902-1968) and developed in the form of a holistic theory. This therapy is based on a combination of recent experimental advances in assessment, psychological - physical treatment and rehabilitation (physical movements of neurological rehabilitation), which is effective in the field of neuropsychological and psychiatric interventions. This method takes into consideration the proximity and integration between theoretical and practical knowledge as well the terms of a practical theory. Neurological rehabilitation concepts are used in different dimensions and it is an intervention for those who suffer from neurological disorders.
Comprehensive assessment of mood performance should include an examination focused on the people's mood, laboratory tests and, if possible, other specialized tests and, in some cases, the assessment is psychosomatic. The results of the full evaluation can be considered the basis for finding possible causes of mood dysfunction, concurrent diseases and serve as a starting point for managing dysfunction. Psychotherapy includes psychological training methods (neurological and psychological treatment information for references metacognitive treating is very important.) Methods of dialogue and therapeutic techniques are effective tools that can be adjusted separately and appropriately.
Interpersonal processes, such as therapeutic alliance, modifying discontinuities and medical treatment validation are required to achieve positive results. Also creative methods like: stories, poetry, music, painting and drawing and playing roles are therapeutic tools to achieve different goals. All of these frequently used methods sound helpful for many patients.
Neurological rehabilitation applications have been practiced in the form of integrated and stand-alone treatments for chronic depression and its effectiveness has been evaluated, but any of its therapeutic techniques or methods have been studied as independent therapy in the treatment of mood disorders.
Vynksy and Cerney in a study represented the effects of this independent treatment to improve executive functions in patients with chronic depression. The results of researches by Pinto Geuveia, indicated this method efficacy in reducing anxiety, tension, anxiety sensitivity and improving symptoms of depression and executive functions in depressed patients.
Based on available evidences and considering the weak points and strengths, this study seeks to examine the effectiveness of schema therapy integrated with neurological rehabilitation methods to reduce early maladaptive schemas and symptoms of chronic depression in patients with chronic depression.
Method
The research method used in this study is a pilot test with single case and multiple baselines. In these pilot projects, test variables are just applied for one person, behavior or situation (after the baseline). This can be used for one person or a small group.
Community, samples and sampling
The research community includes the patients with chronic depression who attended the counseling and psychotherapy department in a teachers specialized clinic, situated in 13th district. The samples are from men and women who had chronic depression and were referred to this center in Tehran, in 1393. They were selected by "convenience sampling". Finally, after patients referral based on entering criteria to the study and doing the Structured Clinical Interview to diagnose (SCID) I axis disorder, the patients were checked out relating exiting criteria by psychiatrists.
After selecting the 6 subjects regarding the pilot project, each time two participants entered the baseline stage simultaneously into third, eighth and twelfth sessions. The method was in a way that every 6 subjects participated in baseline stage and subsequently entered the stage integrated with neurological rehabilitation methods. The following tools were used to collect data in this study:
Structured clinical interview for axis I disorders (SCID-I)
The interview is a flexible tool developed by First et al. Sharifi et al. translated the interview into Persian and conducted it on 299 subjects. Diagnostic agreement for most specific and overall diagnosis was average or effective (Kappa above 60%). General agreement (total current diagnose Kappa was 52% and an overall lifetime diagnose was 55%) obtained was also satisfactory.
Beck depression inventory (BDI- II)
Beck Depression Inventory was proposed to measure depression [11]. This version is more consistent with DSM-IV compared to the first edition, as the BDI, BDI-II has 21 questions (from 0 to 3) and covers all aspects of depression based on cognitive theory. The overall score is variable between 0 and 63, the scores from zero to 13 show minor depression or no depression, 14 to 19 mild depression, 20 to 28 moderate depression and 29 to 63 indicate severe depression. Beck, Steer and Brown studies showed that the questionnaire has high internal consistency. Other studies reported internal consistency of this scale (Cronbach's alpha = 0.93) and retested reliability of (r=0.93).
Young schema questionnaire, long form 232 q. (YSQ-LF-232)
Young Schema Questionnaire [14], first was designed to evaluate early maladaptive schemas by Young and Brown in 1990, and was revised in 1994. The questionnaire was standardized on a sample of 513 students that Cronbach's alpha was 18 on desirable scale between 0.79 to 0.93 (Fata and Dobson, being published). The test results were 0.67 to 0.84 based on retests with intervals of 15 days done for 18 schemas. The questionnaire has satisfying face and judgment validity (according to the same reference). Several studies have shown its effectiveness in classifying patients based on early maladaptive schemas [3].
In this research, the techniques were used to assess early maladaptive schemas in three groups of participants.
Method
In this study, after proving the diagnose of chronic depression by the therapist, patients are being practiced under the treating intervention which is schema therapy integrated with neurological rehabilitation. It is done after getting the consent of patients and explaining the project to them.
Therapy sessions are held for 15 weekly sessions of 60 minutes. At the beginning of the study, all the patients had to complete their research tools. Then the schema therapy for chronic depression was practiced and followed for almost 2 months to determine the stability of the therapeutic effects. The criteria for precluding the patients from treatment process was two successive absence from the sessions. Eligible research subjects were selected from the men and women who attended the clinic (Tehran East Branch of Teachers Clinic). Then the participants were under the practice of interventions. After the third, eighth, twelfth sessions and also at the end of the therapy sessions all were tested and there was a final two- month follow up.
In this study, data analysis is done on the basis of charts review and impact factor methods. The formula used to calculate the percentage of recovery is:
MPI = [(Baseline Mean – Treatment Phase Mean) / Baseline Mean] × 100
Recovery Percentage Formula is a method to measure progress in reducing the problems clients are targeted. This formula was used by Schwars & Blanchard. In this Formula, we subtract the pretest score from the score in post-test then divide the result by the pretest score. If the answer shows at least 50 percent improvement in terms of results can be considered clinically significant.
As you see in Table 1, scores of the first to sixth person in the treatment method of schema therapy integrated with neurological rehabilitation using Beck Depression Scale showed that the first subject’s scores relatively improved at post-treatment (score 12), second and third subject’s scores also relatively improved (to scores 10 and 8). The fourth, fifth and sixth subjects showed a complete improvement (6, 6 and 7). The overall data proves that the method of treatment in which schema therapy is integrated with neurological rehabilitation has lowered the subjects scores.
| Subjects |
Base line |
3rd session |
8th session |
12th session |
Post treatment |
Intervention average |
Follow up session |
Recovery percentage |
Reduction percentage |
| S1 |
37 |
24 |
18 |
15 |
12 |
17.25 |
9 |
53.37 |
114.49 |
| S2 |
39 |
32 |
23 |
17 |
10 |
16.25 |
10 |
58.33 |
140 |
| S3 |
47 |
36 |
25 |
14 |
8 |
20.75 |
9 |
55.85 |
126.5 |
| S4 |
36 |
22 |
18 |
14 |
6 |
15 |
7 |
58.3 |
140 |
| S5 |
43 |
26 |
20 |
15 |
6 |
16.75 |
10 |
61.04 |
156.67 |
| S6 |
45 |
30 |
21 |
12 |
7 |
17.5 |
8 |
61.11 |
157.14 |
Table 1: Subjects scores in Beck Depression Scale at baseline, in- treatment, post-treatment and follow-up process.
Based on the table, the six subjects’ scores in Beck Depression Scale has decreased during the sessions. This issue signifies the efficacy of schema therapeutic methods integrated with neurological rehabilitation in reducing symptoms of depression. This improvement can be observed on the basis of the recovery rate from the first subject to the sixth in turn: (53.37, 58.33, 55.85, 58.3, 61.04, 61.11). Since the scores over 50 percent show treatment efficacy, so it can be concluded that schema therapy integrated with neurological rehabilitation methods has been successful (Figure 1).
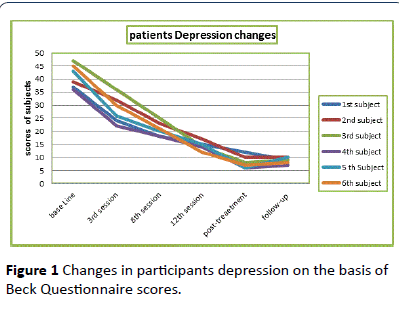
Figure 1: Changes in participants depression on the basis of Beck Questionnaire scores.
| Subjects |
Base line |
3rd session |
8th session |
12th session |
Post treatment |
Intervention average |
Follow up session |
Recovery percentage |
Reduction percentage |
| S1 |
825 |
669 |
443 |
286 |
234 |
408 |
228 |
50.54 |
102.2 |
| S2 |
813 |
596 |
414 |
286 |
227 |
388.5 |
224 |
52.21 |
109.26 |
| S3 |
841 |
609 |
416 |
295 |
230 |
387.5 |
216 |
53.92 |
117.03 |
| S4 |
944 |
678 |
455 |
333 |
259 |
431.25 |
254 |
54.31 |
118.89 |
| S5 |
971 |
647 |
411 |
316 |
265 |
409.75 |
262 |
57.8 |
136.97 |
| S6 |
1063 |
740 |
494 |
393 |
308 |
483.75 |
305 |
54.49 |
119.74 |
Table 2: Subjects overall scores in Beck Depression Scale at baseline, in-treatment, post- treatment and follow-up process
As shown in Table 2, scores of the first to the sixth subject in the process of schema therapy integrated with neurological rehabilitation using “Young Schema Therapy Scale” showed that the scores of all six participants at post-treatment stage went down the cut off score (i.e 615). Total obtained data show that treating relating schema therapy integrated with neurological rehabilitation lowers the participants scores. According to the table, six subjects scores in Young Schema Scale has been decreased which proves the efficacy of this treatment in reducing symptoms of depression. And the issue can be better understood referring the recovery index based on “Young Schema Scale” for the first to the sixth participants which in turn equal (50.54, 52.21, 53.92, 54.31, 57.80, 54.49). Since the scores over 50 percent show treatment efficacy, so it can be concluded that schema therapy integrated with neurological rehabilitation methods has been successful (Figure 2).
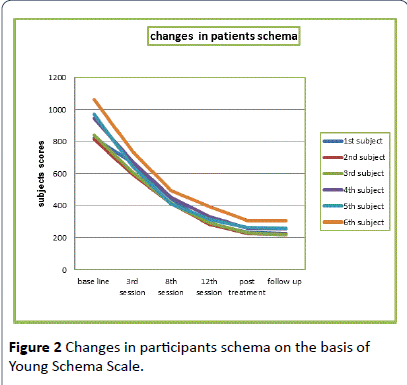
Figure 2: Changes in participants schema on the basis of Young Schema Scale.
Conclusion
The aim of this study was to evaluate the effectiveness of schema therapy integrated with neurological rehabilitation methods to reduce early maladaptive schemas and symptoms of chronic depression in patients with chronic depression. The results showed that treating through this method significantly reduces early maladaptive schemas and symptoms of chronic depression in patients with chronic depressive disorder. The results of this study is consistent with the results of researches from Miller et al., and Schramm et al. [12,13]. To justify these findings, we can say: one therapeutic strategy in schema therapy is experimental strategies to provide the greatest changes in the schema.
Patients can link their cognitions regarding bad schemas to emotional beliefs using experimental techniques. In contrast to cognitive and behavioral techniques with high repetition and practice that follow small changes, changes due to experimental techniques are more significant [15]. Local and foreign researches confirm that the schema therapy resolves many personal and interpersonal problems. Schemas help people explain their deep problems precisely and organize them understandably. The therapist helps the patient to keep track of schema with an emphasis on affections from childhood up to now. In this way, one can find his/her problems, and as a result get out of them while having more motivation for improvement.
Schema therapy can prevent cognitive distortions that misinterpret the environment and can strengthen the schemas. These cognitive distortions can achieve kinds of information which is harmonious with the person’s schema and in terms of emotions, they maintain painful emotions associated with painful schemas, and seek to replace them with positive thoughts.
Schema therapy and its integration with neurological rehabilitation procedures can inhibit and limit self-damaging patterns and involving the patients in these patterns. Also, this treatment can prevent the person to choose situations which maintain schemas and finally the person tries to show positive feedbacks to environment.
In fact, in schema therapy the therapists are seeking "schema restoration".
Repairing schemas means every memory, thought or feeling that can repair schema. Since schemas are resistant to any change, repairing schemas needs great motivation and fighting and also regularity in practice.
The final aim in schema therapy is schema restoration. Since schema includes memories, physical senses and cognitions, so all these components should be repaired in schema restoration process. Schema changes also include changes in behavior, and teaches patients how to replace healthier and more compatible behavior patterns with maladaptive opposing ones [16].
One of the present study limitations was its style of convenient sampling that causes doubts regarding reliability in the process of generalizing results. Another limitation was the short follow-up period. Due to the chronic nature of depression, it is likely that patients who are receiving treatment after a follow-up period cannot maintain therapeutic achievements.
Regarding the effectiveness of treatments based on schema therapy integrated with neurological rehabilitation, it is recommended that psychologists and counselors take advantage of this approach for treating patients with chronic depression. Also, it is suggested that public educational and health programs be offered on the basis of this treatment at all levels in society.
9846
References
- Anderson RL, Klein DN, Riso LP, Ouimette PC, Lizardi H, et al. (1996). The subaffective-character spectrum subtyping distinction in primary early-onset dysthymia: a clinical and family study. J Affect Disord 38: 13-22.
- Young JE (2007) Early Maladaptive Schemas In Chronic Depression. In riso(Eds) Chronic Depression Guilford press, New York, USA.
- Young J, Norman S, Thomas J (1995) Schema Questionnaire. J Cognitive Ther Res 19: 95- 321.
- Butler G, Fennell M,Robson D, GelderM (1991) Comparison of behavior therapy and cognitive–behaviour therapy in the treatment of generalized anxiety disorder. J Consult ClinPsychol 59: 167-175.
- Barlow D,Craske M, Cerney JA, Klosko JS (1989) Behavioral treatment of panic disorder. Behavior Therapy 20: 261-268.
- Gelernter CS,Uhde TW,Cimbolic P, Arnkoff DB,Vittone BJ, et al. (1991) Cognitive–behavioral and pharmacological treatments of social phobia:A controlled study. J Arch Gen Psychiatry 48: 938-945.
- Heimberg RG (1990) Cognitive behavior therapy (for social phobia). In Bellack AS, Hersen M (Eds) Comparative handbook of treatments for adult disorders. Wiley, New York, USA. 203-218.
- Agras WS, Rossiter EM, Arnow B, Schneider JA, Telch CF, et al. (1992) Pharmacologic and cognitive–behavioral treatment for bulimia nervosa: A controlled comparison. Am J Psychiatry 149: 82-87.
- Fairburn CG, Jones R, Peveler RC, Carr SJ, Solomon RA, et al. (1991) Three psychological treatments for bulimia nervosa. A comparative trial. Arch Gen Psychiatry 48: 463-469.
- Baucom D, Sayers S, Scher T (1990) Supplementary behavioral marital therapy with cognitive restructuring and emotional expressivenes training: An outcome investigation. J Consult ClinPsychol 58: 636-645.
- Woody GE, Luborsky L, McClellan AT, O’Brien CP, Beck AT, et al. (1983) Psychotherapy for opiate addicts: Does it help. Arch Gen Psychiatry 40: 1081-1086.
- Miller IW, Norman WH, Dow MG (1986) Psychosocial characteristics of "double depression". Am J Psychiatry 143: 1042-1044.
- Schramm E, Schmeider D, Zobel I, Van Calker D, Dykierek P,et at. (2008) Efficacy of Interpersonal Psychotherapy Plus Pharmacotherapy in chronically depressed inpatients. J Affect Disord 109: 65-73.
- Young JE, Weinberger AD, Beck AT (2001) Cognitive therapy for depression. Clinical handbook of psychological disorders, Guilford press, NewYork, USA. 962-802.
- Thimm JC (2010) Personality and early maladaptive schemas: a five-factor model perspective. J BehavTherExp Psychiatry 41: 373-380.
- Young JE, Klosko JS, Weishaar ME (2003) Schema Therapy: A practitioners Guide. The Guilford press, New York, USA.

