Keywords
Obesity; Diabetes; Hypertension; Association; Statistical analysis
Abbreviations
H. pylori: Helicobacter pylori; BMI: Body Mass Index; BSR: Blood Sugar Random; IgG: Immunoglobulin G; Kg: Kilogram; mmHg: millimeters of Mercury; mg/dl: milligrams per deciliter; CI: Confidence Interval
Introduction
Helicobacter pylori is a well-known pathogenic bacteria associated with the human stomach. More than 50% of the world population is infected by this bacterium and it is more frequent in developing countries [1]. H. pylori infection is a potential risk factor for several other diseases such as chronic gastritis, peptic ulcer, gastric cancer and Mucosa-Associated Lymphoid Tissue (MALT Lymphoma) [2]. It is also considered as class I carcinogen that can induce chronic inflammation [3]. H. pylori infection induces the proliferation of CD4+ T lymphocytes. These lymphocytes recognize the epitope of H. pylori which are structurally similar to those of H+/K+-ATPase. In the absence of peripheral tolerance, a Th1-driven autoreactive clone is activated when dendritic cells present these epitopes to naïve T cells [4]. H. pylori infection induces the secretion of cytokines, CRP, angiotensinogen, free fatty acid, and leptin hormones and thus reactive oxygen species begin to accumulate that cause chronic inflammation [3]. H. pylori infection is suspected to be associated with extra digestive diseases, such as cardiovascular, neurological and metabolic diseases including obesity, diabetes, and hypertension [5].
Obesity is a multifactorial, major public problem that is increasing as well is important globally. Obesity described as the accumulation of extra fats under the skin throughout the body that is sufficient to adversely affect health and reduce life expectancy [6]. Several other health problems which are associated with obesity are hypertension, diabetes, hypoventilation, back and joint pain issues, cardiovascular diseases and gastroesophageal reflux disorder [7]. The prevalence of obesity in Pakistan is 4.8% where as 20.8% population is overweight according to WHO statistics 2016 [8]. H. pylori infection stimulates the excessive release of pro-inflammatory cytokines, such as interleukin (IL-6, IL-8, IL-1B, and TNF-a). The release of pro-inflammatory cytokines causes chronic inflammation, which further leads to the deterioration of insulin resistance and lipid dysmetabolism. Both insulin resistance and lipid dysmetabolism contribute significantly to obesity. Besides, H. pylori infection induces a decrease in the production and secretion of the orexigenic hormone ghrelin. Ghrelin, as a multifunctional polypeptide secreted from gastric mucosa, is involved in ingestion, appetite, and nutrition, especially lipid absorption and lipogenesis [3]. Ghrelin is primarily secreted from the stomach and implicates in the coordination of eating behavior and weight regulation. Circulating ghrelin levels are decreased in human obesity, suggesting a potential association of ghrelin with obesity. Moreover, H. pylori-infected subjects have lower serum leptin levels. The decrease in serum leptin levels could stimulate appetite, and overfeeding may result in overweight and obese. Therefore, obesity and H. pylori infection may interact with each other and form a large complex [9]. Hormone ghrelin exerts long-term appetite-stimulating behavior through its receptors in the hypothalamic paraventricular and arcuate nuclei. Decreased exposure to H. pylori results in increased ghrelin and downregulated gastric leptin in children and in adults, thus increasing appetite-stimulating behavior and leading to obesity. Interestingly, ghrelin has storage in abdominal white adipose tissue. H. pylori could be an indicator of changes in the gut microbiome. It reflects the complex interaction between microbes and the immune system. When H. pylori are eradicated (other microbes will be influenced as well), the inner balance of microbes, appetite-related hormones, and the immune system will be broken, and the person will become obese [10] (Figure 1).
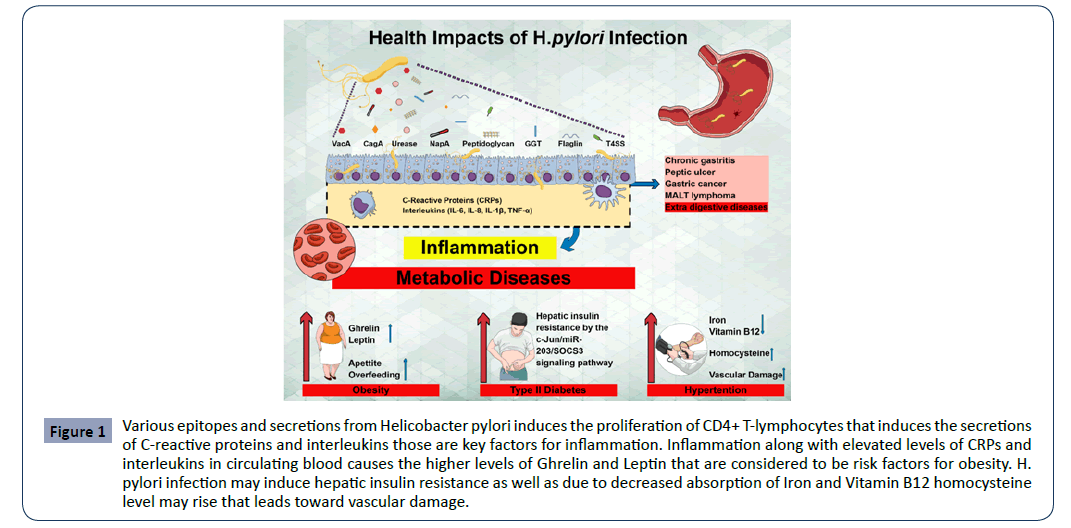
Figure 1: Various epitopes and secretions from Helicobacter pylori induces the proliferation of CD4+ T-lymphocytes that induces the secretions of C-reactive proteins and interleukins those are key factors for inflammation. Inflammation along with elevated levels of CRPs and interleukins in circulating blood causes the higher levels of Ghrelin and Leptin that are considered to be risk factors for obesity. H. pylori infection may induce hepatic insulin resistance as well as due to decreased absorption of Iron and Vitamin B12 homocysteine level may rise that leads toward vascular damage.
Type 2 Diabetes mellitus is another one of the most important causes of morbidity, mortality, and burden on health-system worldwide. Type 2 diabetes mellitus is more prevalent and is characterized by hyperglycemia and a combination of impaired insulin secretion and insulin resistance [11]. According to the World Health Organization (WHO) estimated 422 million people suffered from diabetes [12]. The prevalence of diabetes in Pakistan is 26.3% [13]. H. pylori infection increases the risk of diabetes is not clear, it is biologically plausible. H. pylori infection induces inflammation, and inflammation is suspected to cause diabetes. Besides the inflammatory pathway, it was suggested that H. pylori infection can affect the regulation of ghrelin and leptin. H. pylori infection induces hepatic insulin resistance by the c-Jun/miR-203/SOCS3 signaling pathway [1]. There is an immediate immune response with a production of proinflammatory substances such as cytokines, eiscosanoids and acute-phase proteins during infection that may have effects on extra digestive sites. Many vasoactive substances and cellular mediators, such as tumor necrosis factor alpha (TNF-a) and other cytokines are produced in the gastric mucosa in response to H. pylori infection. These mediators may be transported in the bloodstream and may promote an inflammatory response in organs distant from stomach (Figure 1).
It is said that H .pylori infection plays a role in some endocrine disorders such as autoimmune thyroid disease, diabetes, and primary hyperparathyroidism and may have a high prevalence among patients with diabetes [14]. Insulin resistance can develop in the presence of inflammation or as a result of alterations in counter-regulatory hormones that affect insulin, H. pylori infection may thus promote insulin resistance by inducing chronic inflammation and affecting insulin-regulating gastrointestinal hormones [14]. The Ghrelin can also modulate insulin sensitivity and stimulate insulin-induced glucose uptake, and the H. pylori infection can impair Ghrelin synthesis [3].
High blood pressure or hypertension is another leading risk factor for global mortality and is estimated to have caused 9.4 million deaths and 7% of disease burden [15]. The detection, treatment, and control of hypertension are low especially in developing countries such as in Pakistan leading to swear conditions such as stroke and heart and renal failure. The prevalence of hypertension in Pakistan is 46.2% [16]. H. pylori infection and peptic disease likely affect gastric physiology, including alterations in metabolic hormones (eg, ghrelin and leptin) and micronutrient absorption such as iron and vitamin B12. Vitamin B12 deficiency leads to increased homocysteine concentration and causes vascular damage [17]. The infection with H. pylori has a positive association with high LDL, low HDL, and cardiovascular disease and successful H. pylori eradication decreased the risk of high LDL and low HDL [3].
Metabolic diseases like obesity, type 2 diabetes, and hypertension, an outcome of Helicobacter pylori infection is a major discussion in the recent past. To determine the onset of these diseases in infected individuals could clear the fog in this domain. The major objectives of the study were to find the prevalence of H. pylori infections in the Rawalpindi region and to identify the association between metabolic diseases such as obesity, diabetes, and hypertension.
Materials and Methods
Ethics statement
All individuals signed informed consent prior to their enrollment in the study stating that their data could be used in future medical research. Also, the study was planned according to the ethical guidelines provided by the ethical committee of the Capital University of Science and Technology, Islamabad.
Subjects and clinical data
The cross-sectional study was carried out from May 2017 to August 2017 at several regions of Rawalpindi district, Pakistan. Inclusion criteria were complete age range 18 to 70 years, with no visible physical and mental disability, no pregnancy, Exclusion criteria were the age range below 18 and above 70 years, physically and mentally unfit or disabled persons, having pregnancy in case of female subjects. Socio-demographic information of participants having “a similar socioeconomic status, judged by work type and level of instruction was collected on properly designed data acquisition form. Informed consent was obtained from all participants.
Sample size
The sample size was calculated by using formula Sample Size = Z2 * P (1-p) /e2
Z2 * P (1-p)/e2 N
Where N is the size of the population, e is the margin error and Z is z-score of the number of standard deviations [18]. An estimated sample size of 192 subjects was calculated using the above formula with a 7.1% margin, 95% level of confidence and 1.96 z-score. In this study, 200 total samples were collected. Finally, 192 subjects 105 females and 87 males were enrolled.
Evaluation of H. pylori infection status
One step H. pylori test was performed on-site. The one-step H. pylori test device (Standard diagnostic, Inc. Korea) was used to detect IgG type antibodies to H. pylori in the blood to aid in the diagnosis of H. pylori infection in the laboratory. This test is a rapid chromatographic immunoassay for the qualitative detection. This test was used to identify the subjects that were suffering from H. pylori infection or they were infected with H. pylori infection in the recent past.
Evaluation of obesity infection status
Standing height and body weight were recorded without shoes with light clothing for all subjects. BMI was calculated as weight divided by height squared. Normal weight, overweight, and obesity were defined as BMI <24, 24-30, >30 Kg/m2 respectively [8].
Evaluation of diabetes infection status
Blood sugar random BSR levels were detected by Fingerstick procedure using the device “EasyGlucometer Code C25”. Blood sugar was measured by Type II Diabetes Mellitus was defined as a random plasma glucose of 200 mg/dl or greater [11].
Evaluation of hypertension infection status
Blood pressure was measured in the right arm using a mercury sphygmomanometer after 20 min of rest with the participants in a sitting position. The first and fifth Korotoff sounds were used as systolic and diastolic blood pressure. Hypertension was defined as participants having systolic blood pressure (SBP)>140 mmHg and/or diastolic blood pressure (DBP) >90 mmHg.
Clinical examination
All subjects were interviewed regarding current health status (diabetes mellitus, hypertension, eating disorder, and medication for obesity, diet plan to control obesity, minor surgeries and medication used for other diseases). Blood samples and anthropometric parameters including body height, body weight, body mass index (BMI) and blood pressure were measured or calculated for all participants.
Statistical analysis
Results “were presented as mean ± standard deviation and” percentage. The Wilcoxon Rank Sum test was used for comparison of continuous data, while the chi-square test was used for comparison of categorical variables. Odds ratios and 95% CI values were calculated by” descriptive statistics and risk factor was judged. Chi-square analysis was used to determine the factors that were associated with diseases (obesity, type 2 diabetes mellitus, and hypertension). “Significance was defined as p>0.05. Correlation between H. pylori and obese individuals is judged with respect to calculated BMI. In the next step correlation between infected diabetic and non-diabetic individuals was judged. Association was also checked between hypertension and H. pylori infection. The “statistical analysis was carried out” by “using Statistical Package for Social Sciences (SPSS) Version 20”. Prevalence in the form of percentage was obtained using MS Excel.
Results
Population characteristics and metabolic measures
Out of the total 192 subjects, 55% (105) were females and 45% (87) were males. Obese and Control groups mean age was 38.18 years, minimum 17 years and maximum 85 years with a standard deviation of 14.546. The mean weight obtained was 71.10 Kg with a standard deviation of 15.484. Mean height was observed 63.70 inches with a standard deviation of 3.959. Systolic blood pressure varies from 100 mmHg to 170 mmHg with a mean value of 126.11 mmHg and a standard deviation of 14.725. Diastolic Blood pressure varies from 60 mmHg to 110 mmHg with a mean value of 82.97 and a standard deviation of 8.396. Minimum Blood Sugar Random (BSR) was observed 61 mg/dl and the maximum was 600 mg/dl with a mean value of 146.04 and a standard deviation of 104.164 (Table 1). Prevalence of Helicobacter pylori infection according to sociodemographic factors is shown in (Tables 2 and 3).
Table 1 Characteristics of study participants.
| |
N |
Minimum |
Maximum |
Mean |
Std. Deviation |
| Age |
192 |
18 |
85 |
38.18 |
14.546 |
| Weight (Kg) |
192 |
44 |
160 |
71.10 |
15.484 |
| Height (Inches) |
192 |
49 |
78 |
63.70 |
3.959 |
| Body Mass Index (BMI) |
192 |
16.0 |
53.2 |
27.368 |
6.2519 |
| Systolic BP (mmHg) |
192 |
100 |
170 |
126.11 |
14.725 |
| Diastolic BP(mmHg) |
192 |
60 |
110 |
82.97 |
8.396 |
| Blood Sugar Random (mg/dl) |
192 |
61 |
600 |
146.04 |
104.164 |
Inclusion criteria: Healthy persons minimum age of 17 years, with no any physical disability
Exclusion criteria: Pregnant women, disabled/ mentally or immunologically compromised individuals, individuals under 17 years of age
N is total number of subjects
Table 2 Prevalence of metabolic diseases.
| Diseases/Prevalence |
Prevalence |
Prevalence in Males |
Prevalence in Females |
| H. pylori Infection |
44% |
16% |
29% |
| Obesity |
28% |
5% |
23% |
| Diabetes |
18% |
8% |
10% |
| Hypertension |
22% |
8% |
14% |
*Prevalence of Helicobacter pylori, obesity, diabetes, hypertension for the population of Tehsil Kahuta, District Rawalpindi, Pakistan
*Sample size 192 comprising 87 males, 105 females
BMI normal range: 18.5-24.9, Overweight 25-29.9, Obese above 30-39.9, BSR normal 80-140 mg/dl Diabetic BSR ≥ 200 mg/dl, Hypertensive blood pressure ≥ 90/140 mmHg, normal < 85/130mmHg, high normal 85-89/130-139 mmHg.
Table 3: Prevalence of Helicobacter pylori infection according to sociodemographic factors.
| Variables |
Total |
H. pylori Positive |
H. pylori Negative |
P-value |
| Age |
192 |
85 |
107 |
0.014 |
| Age Groups |
<18 years (11) |
2 |
9 |
.236 |
| 18-27 years (46) |
17 |
29 |
| 28-37 years (34) |
15 |
19 |
| 38-47 years (53) |
25 |
28 |
| 48-57 years (27) |
16 |
11 |
| 58-67 years (14) |
8 |
6 |
| 68-77 years (5) |
2 |
3 |
| >77 years (2) |
0 |
2 |
| Gender |
Male (87) |
30 |
57 |
0.013 |
| Females (105) |
55 |
50 |
| Height |
192 |
85 |
107 |
0.64 |
| Weight |
192 |
85 |
107 |
0.59 |
| BMI |
192 |
85 |
107 |
0.009 |
| Systolic BP |
192 |
85 |
107 |
0.109 |
| Diastolic BP |
192 |
85 |
107 |
0.054 |
| Blood Pressure |
Low (8) |
6 |
2 |
.001 |
| Normal (142) |
52 |
90 |
| High (42) |
27 |
15 |
| BSR |
192 |
85 |
107 |
0.258 |
| Heart Disease |
Yes (12) |
4 |
8 |
0.431 |
| No (180) |
81 |
99 |
| Eating Disorders |
Yes (90) |
48 |
42 |
0.018 |
| No (102) |
37 |
65 |
| Physical Activity |
Yes (32) |
9 |
23 |
0.044 |
| No (160) |
76 |
84 |
| Education Level |
Nil (58) |
32 |
26 |
.085 |
| Low (37) |
18 |
19 |
| Moderate (72) |
28 |
44 |
| High (25) |
7 |
18 |
| Job Status |
Nil (105) |
47 |
58 |
0.938 |
| Govt. Employee (29) |
12 |
17 |
| Self Employed (17) |
8 |
9 |
| Private Sector (41) |
18 |
23 |
| Marital Status |
Married (144) |
76 |
68 |
0.000 |
| Unmarried (48) |
9 |
39 |
| History of Surgery |
Yes (65) |
25 |
40 |
0.246 |
| No (127) |
67 |
60 |
| Medication to Control Obesity |
Yes (0) |
0 |
0 |
- |
| No (192) |
85 |
107 |
| Medication for any other Disease |
Yes (38) |
18 |
20 |
0.668 |
| No (154) |
67 |
87 |
| Diet Plan for Obesity |
Yes (3) |
0 |
3 |
0.120 |
| No (189) |
85 |
104 |
*Age (years), Age Groups (10 years), Systolic BP, Diastolic BP. Blood Sugar Random (BSR) were measured.
*Question were asked if the subjects had low normal or high blood pressure problem, if they had history of any heart disease, eating disorders, physical activity, history of surgery, medication to control obesity, medication for any other disease, diet plan for obesity. Answers were recorded in the form of Yes or No.
*Education level Nil (No any Education from school), Low (education up to grade 5), Moderate (up to grade 12), High (up to graduation or above)
Status helicobacter pylori infection
In this study, the aim was “to investigate the prevalence of H. pylori infection and its relation with BMI in” subjects of Rawalpindi. “Overall prevalence of H. pylori infection was” observed approximately 44% including both male and female subjects. Out of 192 subjects, 85 people were found seropositive for H. pylori IgG antibody and 102 people were found negative. 85 seropositive people were either currently infected or either had an infection in the past. It was observed that 16% (30) Males out of 192 subjects and 29% (55) female subjects were seropositive for H. pylori infection and 57% (30) males, 26% (50) female subjects from a total of 192 subjects were found seronegative.
Status of obesity
According to WHO BMI classification criteria 5% subjects were underweight, 33% individuals were normal lean 34% were overweight, 16% subjects were categorized as Obese Class I as there BMI was above 25, 7% subjects were under Obese Class II and 4% were categorized under Obese class III as there BMI was greater than 40. All individuals having BMI greater than 30 were considered obese and the prevalence of obesity was observed 28% in subjects of the Rawalpindi region. It was observed that 1% underweight, 9% Normal lean Individuals 9% Overweight and 13% obese subjects were seropositive for H. pylori IgG. Among obese class-I, 43% subjects were infected and 57% of individuals were not infected similarly among obese class-II and obese class III 64% & 37% of subjects were infected and 36% & 63% were found negative.
Status of diabetes
Diabetes is another increasing health problem worldwide as well as in Pakistan. The prevalence of diabetes was observed 18 % as 35 individuals out of 192 were diabetic. H. pylori infection in diabetic subjects was 9% positive and 9% negative. Similarly, 35% positive and 48% negative for non-diabetic subjects.
Status of hypertension
22% of subjects were observed patients of Hypertension (high blood pressure). 74% of subjects were normal with no blood pressure complaints only 4% of subjects were observed with low BP complaints. 3%, 27%, and 14% of subjects were found infective for subjects having low, normal and high blood pressure. 1%, 47%, and 8% were not infective among subjects having low, normal and high blood pressure (Table 2). Comparison of metabolic diseases in H. pylori positive and H. pylori negative groups is shown in (Table 4).
Table 4 Comparison of metabolic diseases in H. pylori positive and H. pylori negative groups.
| Variables |
Total |
H. pylori Positive |
H. pylori Negative |
P-value |
| Obesity |
Obese (54) |
30 |
24 |
0.049 |
| Non Obese (138) |
55 |
83 |
| Diabetes |
Non Diabetic (157) |
67 |
90 |
0.346 |
| Diabetic(35) |
18 |
17 |
| Hypertension |
Hypertensive (42) |
27 |
15 |
0.003 |
| Normal (150) |
58 |
92 |
Association of H. pylori with obesity, diabetes, and hypertension
Pearson’s Chi-square is a test for independence or correlation coefficient” and a test for association. For 139 controls and 53 subjects, Chi-square test values for H. pylori and obesity was calculated as 4.513 with a degree of freedom that is equal to 1 and a p-value of 0.034 that showed association is present, Phi and Cramer’s V test values were 0.153 which shows that results are significant. The odds ratio with a 95% confidence interval was obtained as 1.992. For H. pylori and diabetes including 157 controls and 35 subjects Chi-square test values was 0.889 with a degree of freedom that equals to 1 and P-value of 0.346 according to these values, the association was not present, Phi and Cramer’s V test values were obtained as 0.068 which represents less significant results. For 142 controls and 50 subjects Chi-square test values for H. pylori infection and hypertension were obtained 12.938 with a degree of freedom equals to 1 and p-value of 0.00 represents significant association, odd ratio value was 3.360 and Phi and Cramer’s V test values were calculated that were 0.260 (Table 5).
Table 5 Association of Helicobacter pylori infection with metabolic diseases.
| Statistical Analysis |
Total Samples |
Normal |
Diseases |
Chi- square Values |
Degree of Freedom |
P-Value |
Odd Ratio 95% CI |
Phi Values |
Cramer’s V test |
Association |
| Correlation of H. pylori and Obesity |
192 |
138 |
54 |
4.513a |
1 |
0.049 |
1.992 |
0.153 |
0.153 |
Positive and slightly significant |
| Correlation of H. pylori and Diabetes |
192 |
157 |
35 |
0.889a |
1 |
0.346 |
1.422 |
0.068 |
0.068 |
No Association |
| Correlation of H. pylori and Hypertension |
192 |
152 |
42 |
12.938a |
1 |
0.003 |
3.360 |
0.260 |
0.260 |
Positive and slightly significant |
a. 0 cells (0.0%) have expected count less than 5. The minimum expected count is 15.49.
b. Computed only for a 2x2 table
*P-value= <0.05
CI: 95% confidence Interval
Discussion
Mean values of calculated BMI suggests that peoples of Rawalpindi region are overweight and are not obese, systolic diastolic blood pressure is observed normal, blood random sugar levels were observed above them normally. This might be because of the high consumption of soft drinks, juices, tea, and sweets as well as due to no physical activity (walk, exercise, etc.) observed other than workload.
By comparing the infection rate of H. pylori in males and females separately, it was observed that the prevalence was high among female subjects. All seropositive males and females were found symptomatic for disorders like stomach pain, and vomiting, etc. The reason for the high prevalence among females is might be the consumption of market foods as they are not properly washed with clean water before preparation as well as storage conditions are also not proper.
H. pylori infection trend was found increasing from normal to overweight and obese subject (Figure 2A) which was further confirmed by observing H. pylori infection trend among obese class I, obese Class II and obese Class III (Figure 2D). It is clear that the prevalence of H. pylori infection among obese subjects is high than normal lean subjects. Diabetic subjects are more susceptible to various infections due to their suppressed immunologic conditions. However, H. pylori infections among diabetic persons were observed as equal to non-diabetic subjects (Figure 2B). The prevalence of hypertension was calculated 22% whereas 28% obese shows association of weight gain and hypertension as approximately equally increasing. Figure 2C shows that the infection rate is high among persons having high blood pressure or are hypertensive (Figure 2).
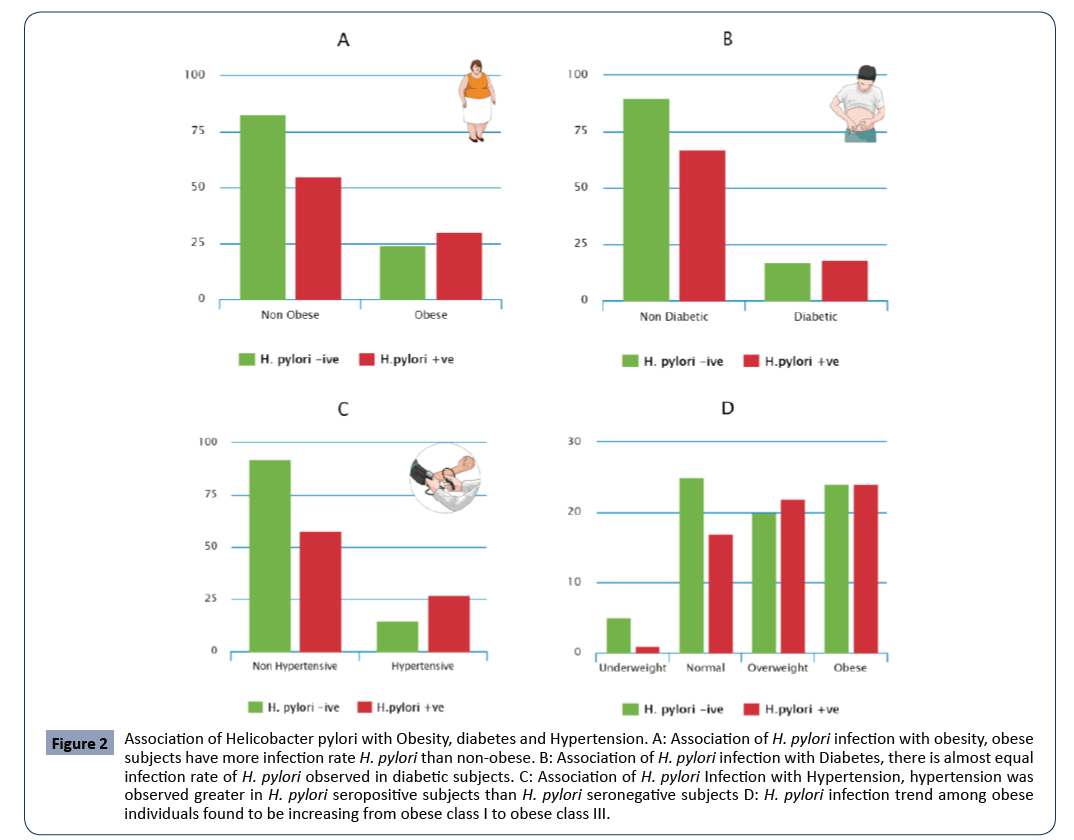
Figure 2: Association of Helicobacter pylori with Obesity, diabetes and Hypertension. A: Association of H. pylori infection with obesity, obese subjects have more infection rate H. pylori than non-obese. B: Association of H. pylori infection with Diabetes, there is almost equal infection rate of H. pylori observed in diabetic subjects. C: Association of H. pylori Infection with Hypertension, hypertension was observed greater in H. pylori seropositive subjects than H. pylori seronegative subjects D: H. pylori infection trend among obese individuals found to be increasing from obese class I to obese class III.
The significant “association between obesity and H. pylori infection was observed as P-value is obtained 0.034 is less than the alpha value 0.05 which means the results are statistically significant in” other words obesity and H. pylori infection are not independent are dependent on each other. There was no significant association between diabetes and H. pylori infection, in other words, diabetes and H. pylori infection are independent as P-value obtained was 0.889 was greater than the alpha value of 0.05 which means the results are statistically not significant. There is a significant association between H. pylori infection and hypertension, in other words, hypertension and H. pylori infection are dependent on each other as P-value obtained were 0.000 is smaller than the alpha value of 0.05 which means the results are statistically significant.
Odd ratio involved for risk suggests that odds for developing obesity 1.992 times greater for “individuals having H. pylori” positive infection compared with H. pylori-negative infections. Odd ratio involved for risk from (Table 5) suggests that odds for developing diabetes 1.422 times greater for individuals having H. pylori-positive infection compared with H. pylori-negative infections. Odd ratio involved for risk from (Table 5) suggests that odds for developing hypertension 3.360 times greater for individuals having H. pylori-positive infection compared with H. pylori-negative infections.
Cramer's “V is a measure of association so it tells us how important findings are” if the value is 0 then no relationship, 0.1 for a low relationship, 0.2 for moderate relationship and 0.3 for a strong relationship. Here for obesity and H. pylori, the value is obtained (Table 5) 0.153 which means there is a moderate relationship between the association of obesity and H. pylori. Phi Values also suggest that there is a relationship present between obesity and H. pylori infection. For diabetes and H. pylori, Cramer's V value is obtained (Table 5) 0.068 which means there is no relationship between the association of diabetes and H. pylori. Phi values 0.068 also suggest that there is no relationship present between diabetes and H. pylori infection. For Hypertension and H. pylori, Cramer's V value is obtained (Table 5) 0.260 which means there is a moderate to a strong relationship between the association of hypertension and H. pylori infections. Phi values 0.296 also suggest that there is a relationship present “between H. pylori infection and hypertension.
Conclusion
“Overall prevalence of H. pylori infection was” observed 44% including both male and female subjects. By comparing the infection “rate of H. pylori in” males and females separately, it was observed that the prevalence was high among female subjects. The prevalence of obesity was observed 28% in subjects of the Rawalpindi region. H. pylori infection trend was found increasing “from normal to overweight and obese” subject which was further confirmed by observing H. pylori infection trend among “obese class I, obese Class II” and “obese Class III”. The prevalence of diabetes was observed 18% as 35 individuals out of 192 were diabetic. Diabetic subjects are more susceptible to various infections due to their suppressed immunologic conditions. However, H. pylori infection among diabetic person were observed as equal to non-diabetic subjects. 22% of subjects were observed patients of hypertension (high blood pressure). The infection rate of H. pylori is observed high among persons having high blood pressure or are hypertensive.
There is a significant “association between obesity and H. pylori infection in” other words “obesity and H. pylori infection are” not independent and are dependent on each other. There is a moderate relationship between the association of obesity and H. pylori. There is no significant association between diabetes and H. pylori infection in other words diabetes and “H. pylori infection are independent”. “There is no relationship between the” association of diabetes “and H. pylori”. There is a significant association between H. pylori infection and hypertension, in other words, hypertension and H. pylori infection are dependent on each other. There is a moderate to a strong relationship between the association of hypertension and H. pylori infections. In conclusion, data suggest that there is a positive relationship of H. pylori infection with obesity, hypertension and inverse relationship “was observed between H. pylori infection and diabetes”.
Large scale studies are required in several regions of Pakistan to check “the prevalence of H. pylori infection”, obesity, diabetes, and hypertension. The various statistical method and study designs can be used to asses association. Studies are required to trace out the mechanisms by which H. pylori induce obesity and hypertension.
Acknowledgment
We gratefully acknowledge and thank full to Dr. Sohail Ijaz Awan MS THQ hospital Kahuta, Dr. Javed Iqbal Soomro M.O THQ hospital Kahuta, Dr. Javed’s Clinic and Saeed Pharmacy for organizing free medical camps and for helping us to collect samples and data.
33229
References
- Kato M, Toda A, Yamamoto-Honda R, Arase Y, Sone H (2019) Association between Helicobacter pylori infection, eradication and diabetes mellitus. J Diabetes Investig 10: 1341-1346.
- Monno R, de Laurentiis V, Trerotoli P, Roselli AM, Ierardi E, et al. (2019) Helicobacter pylori infection: association with dietary habits and socioeconomic conditions. Clin Res Hepatol Gastroenterol 43: 603-607.
- Yang W, Xuan C (2016) Influence of Helicobacter pylori Infection on Metabolic Syndrome in Old Chinese People. Gastroenterol Res Pract 2016: 6951264.
- Wawro N, Amann U, Butt J, Meisinger C, Akmatov MK, et al. (2019) Helicobacter pylori Seropositivity: Prevalence, Associations, and the Impact on Incident Metabolic Diseases/Risk Factors in the Population-Based KORA Study. Front Public Heal 7: 96.
- Zhang Y, Du T, Chen X, Yu X, Tu L, et al. (2015) Association between Helicobacter pylori infection and overweight or obesity in a Chinese population. J Infect Dev Ctries 9: 945-953.
- Pigeyre M, Saqlain M, Turcotte M, Raja GK, Meyre D (2018) Obesity genetics: insights from the Pakistani population. Obes Rev 19: 364-380.
- Zhu Y, Hedderson MM, Quesenberry CP, Feng J, Ferrara A (2019) Central Obesity Increases the Risk of Gestational Diabetes Partially Through Increasing Insulin Resistance. Obesity 27: 152-160.
- Hassan F, Hassan B (2017) Is obesity endemic to Pakistan? J Pakistan Med Assoc 67.
- Xu C, Yan M, Sun Y, Joo J, Wan X, et al. (2014) Prevalence of Helicobacter pylori infection and its relation with body mass index in a Chinese population. Helicobacter 19: 437-442.
- Ness-Jensen E, Langhammer A, Hveem K, Lu Y (2019) Helicobacter pylori in relation to asthma and allergy modified by abdominal obesity: The HUNT study in Norway. World Allergy Organ J 12: 100035.
- Shenoy S, Seixas A, Grandner MA (2019) Obesity, Diabetes, and Metabolic Syndrome. Handb Sleep Disord Med Cond 2019: 153-173.
- Jawed K, Nisar N, Hussain M, Nawab F (2019) A Study Based on Use of Complementary and Alternative Medicine among Diabetic Patients in Karachi, Pakistan. Journal of the Dow University of Health Sciences 13: 10-16.
- Aamir AH, Ul-Haq Z, Mahar SA, Qureshi FM, Ahmad I, et al. (2019) Diabetes Prevalence Survey of Pakistan (DPS-PAK): prevalence of type 2 diabetes mellitus and prediabetes using HbA1c: a population-based survey from Pakistan. BMJ Open 9: e025300.
- Vafaeimanesh J, Bagherzadeh M, Mirzaei A, Parham M, Norouzinia M, et al. (2016) Effect of Helicobacter pylori on metabolic syndrome parameters in diabetic patients. Gastroenterol Hepatol from bed to bench 9: S36-S41.
- Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, et al. (2010) A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380: 2224-2260.
- Basit A, Tanveer S, Fawwad A, Naeem N (2019) Prevalence and contributing risk factors for hypertension in urban and rural areas of Pakistan; a study from second National Diabetes Survey of Pakistan (NDSP) 2016–2017. Clin Exp Hypertens 42: 218-224.
- Shindler-Itskovitch T, Chodick G, Shalev V, Muhsen K (2019) Helicobacter pylori infection and prevalence of stroke. Helicobacter 24: 1-7.
- Charan J, Biswas T (2013) How to calculate sample size for different study designs in medical research? Indian J Psychol Med 35: 121-126.

