Hisashi Ito1, Tazuyo Kawaminami2, Kayo Asano2, Tomoko Fukunaga3, Chiseko Karai4, Satsuki Okuma4, Sachiko Takeshita5, Motokazu Tsutsumi5, Yoshihiro Tokeshi6 and Tetsuya Itagaki7
1Department of Neurology, Shonan Fujisawa Tokushukai Hospital, Fujisawa, Japan
2Healthcare Center, Okinoerabu Tokushukai Hospital, China, Japan
3Department of Rehabilitation, Okinoerabu Tokushukai Hospital, China, Japan
4Department of Nursing, Okinoerabu Tokushukai Hospital, China, Japan
5Department of Radiology, Okinoerabu Tokushukai Hospital, China, Japan
6Department of Internal Medicine, Okinoerabu Tokushukai Hospital, China, Japan
7Department of Neurosurgery, Naze Tokushukai Hospital, Amami, Japan
*Corresponding Author:
Hisashi Ito
Department of Neurology
Shonan Fujisawa Tokushukai Hospital
251-0041, Fujisawa, Japan
Tel: +81-466-35-1177
E-mail: hisashi.ito@tokushukai.jp
Received Date: September 19, 2018; Accepted Date: October 25, 2018; Published Date: October 29, 2018
Citation: Ito H, Kawaminami T, Asano K, Fukunaga T, Karai C, et al. (2018) The Prevalence of Unruptured Cerebral Aneurysms in Okinoerabu: A Japanese Hospital-Based Study. J Neurol Neurosci Vol.9 No.5:273. DOI: 10.21767/2171-6625.1000273
Keywords
Unruptured cerebral aneurysms; Prevalence; MR Angiography
Introduction
Most unruptured cerebral aneurysms (UCAs) are asymptomatic and we often identify them incidentally; however, it is important to detect UCAs by various techniques to prevent subarachnoid hemorrhage. In this study, we investigated the prevalence of UCAs on Okinoerabu, a small island in Japan, using MR angiography (MRA) with 1.5-Tesla MRI.
Materials and Methods
This was a retrospective study of adult residents of Okinoerabu who underwent examination of the brain using MRA, called ‘Brain Dock’. The examination was performed at Okinoerabu Tokushukai Hospital from December 2017 to May 2018. The Review Board of Okinoerabu Tokushukai Hospital Ethics Committee approved this study. Distributions of the age and sex are shown in Table 1. We collected their past medical histories including smoking, hypertension, diabetes, and hyperlipidemia.
| Variables |
Men |
Women |
| Age range (Yr) |
No of persons |
No of UCAs+ |
No of persons |
No of UCAs+ |
| 20~29 |
3 |
0 (0%) |
4 |
0 (0%) |
| 30~39 |
8 |
1 (12.5%) |
11 |
0 (0%) |
| 40~49 |
11 |
0 (0%) |
16 |
0 (0%) |
| 50~59 |
13 |
1 (7.7%) |
27 |
4 (14.8%) |
| 60~69 |
41 |
2 (4.9%) |
89 |
8 (9.0%) |
| 70~79 |
38 |
4 (10.5%) |
62 |
4 (6.5%) |
| 80~ |
10 |
1 (10.0%) |
23 |
2 (8.7%) |
| Total |
124 |
9 (7.3%) |
232 |
18 (7.8%) |
| |
Table 1: The age- and sex-distribution and the prevalence of UCAs in 10-year age groups.
We performed multislab 3-dimensional time-of-flight MRA of the brain (repetition time, TR 28.0 msec; echo time, TE 7.0 msec; thickness 0.6 mm) using a 1.5-Tesla MRI (Magnetom Essenza, Siemens Healthcare K.K.). Neuroradiologically experienced neurologist and neurosurgeon interpreted MRA. UCAs that were 2.0 mm or more in their largest dimension were included in the study. On the other hand, we excluded fusiform or dissecting aneurysms from the analysis because of differences in pathological origins. We evaluated the overall, age-specific, and sex-specific prevalence.
We classified the locations of UCAs as: internal carotid artery (ICA), middle cerebral artery (MCA), anterior cerebral artery (ACA, including the anterior communicating artery), posterior cerebral artery (PCA, including the posterior communicating artery), and vertebrobasilar artery (VA-BA). In addition, we classified UCAs into five size categories (less than 3.0 mm, 3.0 to 4.9 mm, 5.0 to 6.9 mm, 7.0 to 11.9 mm, and more than 12.0 mm).
The chi-square test and Mann-Whitney U-test were used for statistical analysis. All P-values were two-sided and considered significant if they were 0.05 or less.
Results
Thirty UCAs were identified in 27 of 356 persons (Men 124; Women 232; 22 to 91 years, 63.9 ± 13.3 years). Among them, multiple UCAs were discovered in 3 persons. The overall prevalence was 7.6% with 7.3% for men and 7.8% for women. UCAs were identified in those aged over 50 except for one person (96.3%). The prevalence of UCAs increased with age in men, and it was the highest in the 5th decade in women (14.8%). There was no significant difference in age, sex, smoking, or comorbidity between the groups with and without UCAs (Tables 1 and 2). The most common location of UCAs was ICA (56.7%), followed by VA-BA (23.3%). The most common maximum diameter was 3.0 to 4.9 mm (56.7%), and most of the UCAs were less than 4.9 mm (93.4%) (Figure 1).
| Characteristics |
UCAs+ (n=27)
|
UCAs- (n=329)
|
Total (n=356)
|
P value
|
| Mean Age (yr) |
67.5 ± 11.4 |
63.6 ± 13.5 |
63.9 ± 13.3 |
0.322* |
| Men / Women (n) |
|
115 / 214 |
124 / 232 |
0.968** |
| Smoking (n) |
5 (18.5%) |
80 (24.3%) |
85 (23.9%) |
0.657** |
| Hypertension (n) |
12 (44.4%) |
137 (41.6%) |
149 (41.9%) |
0.777** |
| Diabetes (n) |
0 (0%) |
36 (10.9%) |
36 (10.1%) |
NE*** |
| Hyperlipidemia (n) |
2 (7.4%) |
64 (19.5%) |
66 (18.5%) |
NE*** |
| |
Table 2: The comparison between UCAs group and non-UCAs group (*Chi-square test; **Mann-Whitney U-test; ***not examined as numbers were too small).
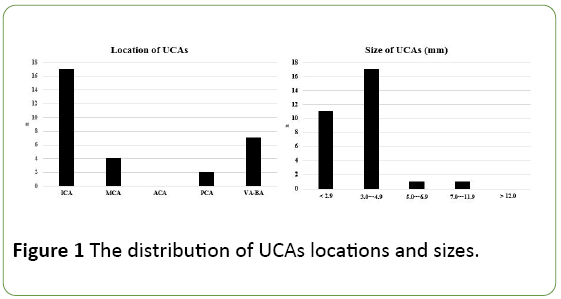
Figure 1: The distribution of UCAs locations and sizes.
Discussion
Okinoerabu is a small island located in the south-west of Japan, and the approximate adult population is 10,000 [1] (Figure 2). Both transportation and medical resources are limited. MR imaging was available only at Okinoerabu Tokushukai Hospital during the study period.
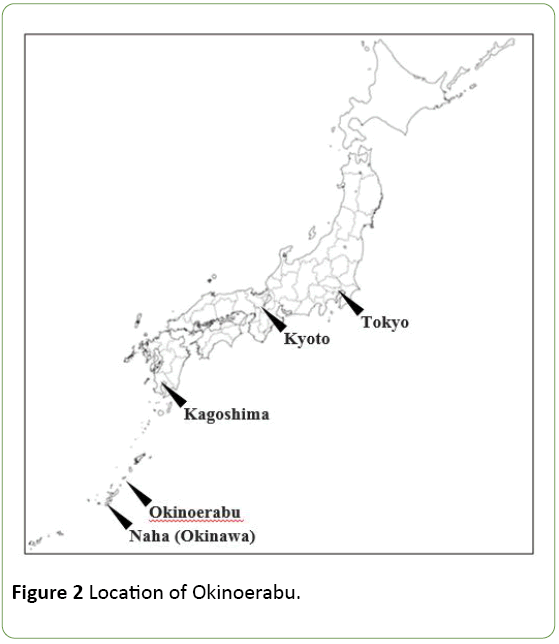
Figure 2: Location of Okinoerabu.
The previously reported prevalence of UCAs in Japan varied widely (Table 3) [2-8]. Ujiie et al. first reported the prevalence of UCAs as 2.7% [2]. Three studies after this one revealed a similar prevalence [4,5,7], while other studies demonstrated a higher prevalence, 4.3% to 8.4% [3,6,8]. They were evaluated by angiography [2,3], autopsy [4], and MRA [3,5-8]. The prevalence of UCAs in angiography studies tended to be higher than that in autopsy and MRA studies [9,10]. On the other hand, Gibbs et al. reported that MRA with 1.5-Tesla and 3- Tesla MR systems could demonstrate all aneurysms that had already been identified by angiography [11]. Recently, MRA has become the most popular tool to detect UCAs as it is a noninvasive and repeatable procedure. A high-tesla MR system could provide better image quality, leading to a higher rate of UCA detection [6,11]; however, the prevalence of UCAs in our study was higher than that using MRA with a 3-Tesla MR system [8]. Therefore, the magnetic field intensity and detection rate of UCAs might not be correlated.
| Author |
Ujiie H et al. [2] |
Nakagawa T et al. [3] |
Iwamoto H et al. [4] |
Horikoshi T et al. [5] |
Igase K et al. [6] |
Harada K et al. [7] |
Imaizumi Y et al. [8] |
Our study |
| No of objects |
1612 |
400 |
1230 |
4518 |
3414 |
8696 |
4070 |
356 |
| Method |
Angiography |
Angiography + MRA |
Autopsy |
MRA (0.5 T) |
MRA (3 T) |
MRA (1.5 T) |
MRA (3 T) |
MRA (1.5 T) |
| Prevalence |
2.70% |
6.50% |
2.20% |
2.80% |
8.40% |
3.20% |
4.30% |
7.60% |
| Common location |
ICA |
ICA |
MCA |
MCA |
ICA |
ICA |
ICA |
ICA |
| Common size |
less than 6.0 mm |
less than 5.0 mm |
ND** |
2.0 to 4.9 mm |
3.0 to 4.9 mm |
2.0 to 4.9 mm |
2.0 to 2.9 mm |
3.0 to 4.9 mm |
| |
Table 3: Previous epidemiological study of UCAs from Japan (*Magnetic flux density was not described; **Not described).
Except for one study [3], the prevalence in women was higher than that in men [2,4-8], which is similar to our results. In addition, several studies from Japan demonstrated that the prevalence of UCAs increased with age [2,5,7,8], and we also recognized this trend in men. We might have to take the age distribution of each study into consideration when evaluating the prevalence of UCAs.Regarding the characteristics of UCAs, both the location and size in our study were similar to those of previous reports from Japan [2,3,6-8], except for the prevalence of VA-BA aneurysms. One advantage of our study is its limited bias because it was performed in a relatively isolated environment.
On the other hand, the limitation of this study is a small size. We have to continue this investigation with more persons to fully consider the characteristics of UCAs on Okinoerabu.
Conclusion
The overall prevalence of UCAs was comparatively high on Okinoerabu. Most of the UCAs were identified in those over 50 years old. ICA was the most commonly affected region, and most UCAs were smaller than 4.9 mm.
Acknowledgements
We thank Dr. Tatsuya Yagi (Department of Radiology, Shonan Fujisawa Tokushukai Hospital) and Dr. Tetsumasa Kamei (Department of Neurology, Shonan Fujisawa Tokushukai Hospital) for their advices to this study.
23649
References
- https://www.pref.kagoshima.jp/ac09/tokei/bunya/kokutyo/h27kokutyo/h27jinnkoutoukihonnsyuukeinennreibetujinnkou.html
- Ujiie H, Sato K, Onda H, Oikawa A, Kagawa M, et al. (1993) Clinical analysis of incidentally discovered unruptured aneurysms. Stroke 24: 1850–1856.
- Nakagawa T, Hashi K (1994) The incidence and treatment of asymptomatic, unruptured cerebral aneurysms. J Neurosurg 80: 217-223.
- Iwamoto H, Kiyohara Y, Fujishima M, Kato I, Nakayama K, et al. (1999) Prevalence of intracranial saccular aneurysms in a Japanese community based on a consecutive autopsy series during a 30-year observation period. The Hisayama study. Stroke 30: 1390–1395.
- Horikoshi T, Akiyama I, Yamagata Z, Nukui H (2002) Retrospective analysis of the prevalence of asymptomatic cerebral aneurysm in 4518 patients undergoing magnetic resonance angiography - When does cerebral aneurysm develop ? Neurol Medico-Chirurgica (Tokyo) 42: 105–112.
- Igase K, Matsubara I, Igase M, Miyazaki H, Sadamoto K (2012) Initial experience in evaluating the prevalence of unruptured intracranial aneurysms detected on 3-Tesla MRI. Cerebrovasc Dis 33: 348–353.
- Harada K, Fukuyama K, Shirouzu T, Ichinose M, Fujimura H, et al. (2013) Prevalence of unruptured intracranial aneurysms in healthy asymptomatic Japanese adults: differences in gender and age. Acta Neurochir (Wien) 155: 2037-2043.
- Imaizumi Y, Mizutani T, Shimizu K, Sato Y, Taguchi J (2018) Detection rates and sites of unruptured intracranial aneurysms according to sex and age: an analysis of MR angiography-based brain examinations of 4070 healthy Japanese adults. J Neurosurg 2018 Apr 6:1-6. [Epub ahead of print]
- Rinkel GJ, Djibuti M, Algra A, Van Gijn J (1998) Prevalence and risk of rupture of intracranial aneurysms: A systematic review. Stroke 29: 251–256.
- Okahara M, Kiyosue H, Yamashita M, Nagatomi H, Hata H, et al. (2002) Diagnostic accurasy of magnetic resonance angiography for cerebral aneurysms in correlation with 3D-digital subtraction angiographic images: A study of 133 aneurysms. Stroke 33: 1803-1808.
- Gibbs GF, Huston J 3rd, Bernstein MA, Riederer SJ, Brown RD Jr (2004) Improved image quality of intracranial aneurysms: 3.0-T versus 1.5-T time-of-flight MR angiography. Am J Neuroradiol 25: 84–87.

