Keywords
Syria; Refugees; Camp health; Evaluation; Services
Introduction
Nowadays, the situation of asylum seekers, refugees reestablished in third countries, and people forced into refugee camps poses as one of the most serious problems for the international community [1]. Since March 2011, Syria has been going through a state of political crisis and instability resulting to an exodus of Syrians to neighboring countries. Following anti-regime demonstrations that began in March 2011 in Deraa, Syria, which then spread throughout the country, a part of the population started to flee the turmoil and seek refuge in neighbouring countries [2]. Over the last 32 months, several thousand dead people have been reported, and the amount of wounded is still unknown. By the end of October 2013, The World Health Organization (WHO) estimated over 2.3 million refugees in Lebanon, Jordan, Turkey, Egypt and North Africa [3-5].
In Jordan the number of the Syrian refugees is estimated around 550.000 and growing every day [6,7]. With up to 3,500 Syrians crossing the borders every day, the rate at which refugees have poured over Syria’s southern border has outstripped the ability of the Jordanian government and the international community to ensure adequate access to health services for refugees living inside Zaatari, the main refugee camp, and those dispersed throughout Jordan [8]. In the beginning of September 2013, UNHCR’s total number for persons of concern in Jordan was 519,676, with 492,526 registered as refugees (Table 1). The coordinated Regional Response Plan for Syrian refugees (RRP) appealed for US$ 1 billion to cover the needs of 1.1 million Syrian refugees in the region from 1 January to 30 June 2013 [9]. According the same research, the indicators of Jordan’s health system capacity has been changed very much (Table 2). Figure 1 shows the visits of Syrian refugees in hospitals and in health centers. There is a huge increase of people visiting the hospitals (less than 1.000 in January 2012, more than 10.000 in March 2013), and health centers (less than 1.000 in January 2012, around 16.000 in March 2013) [8,10].
 Health is a very important factor in the lives of immigrants and their families. The access to good and affordable health services contributes to integration of immigrants into the community more easily, to prevent the inequality, but also to safeguard public health. Access to effective health care, should be considered as important as housing and education [11].
Health is a very important factor in the lives of immigrants and their families. The access to good and affordable health services contributes to integration of immigrants into the community more easily, to prevent the inequality, but also to safeguard public health. Access to effective health care, should be considered as important as housing and education [11].
The target of the majority of the available studies until now on refugees, have been the movement from non-Western to Western countries that have developed immigration policies like US, Germany, Canada, Australia etc. [12,13]. Information on the health status and use of health services by the refugees in Jordan is limited. The purpose of this study is to evaluate the access and services that are provided to the Syrian refugees in Jordan. More specifically, our aim is to explore refugees’ attitudes towards health services (i.e. evaluation of the adequacy of health care services and the degree of their satisfaction by the services provided). We seek to identify the problems that refugees confront and their significance (Table 1 and 2) (Figure 1).
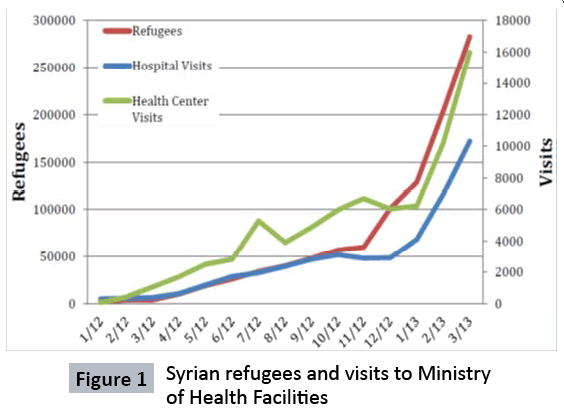
Figure 1: Syrian refugees and visits to Ministry of Health Facilities
Methods
This is a cross-sectional study. Data collection with the use of questionnaires took place from August 1 to October 30, 2013 in Irbid. The area selected for the survey was Irbid (Zaatri camp) since it is the city with the highest Syrian population in Jordan (it is located the border with Syria). The original sample collected by the researchers in the beginning of this survey was 140 subjects. Of them 9 refused to participate, 6 questionnaires were not accepted due to incorrect completion, while 5 persons were excluded due to age criteria (they were under 18 years old). The participation rate was 86%. Questionnaires were administered by a native speaker of the Arabic language, so no language barriers interfered with communication. The final sample size was 120 refugees of both genders. The sampling technique used, was snowball (i.e. Initial approach of immigrants with a wide network of contacts resulted to eventually higher accessibility to new potential participants). The questionnaires were designed by researchers according on the relevant literature [14-18]. The questionnaires consisted of questions concerning demographic information (e.g. age, gender, marital status, education etc.), medical information about the state of their health, and problems they encounter during their stay in the camp, as well as questions related to evaluation of their access to health services (selfreported questionnaires).
Results
Baseline characteristics
Baseline characteristics of people participants are presented in table 3. Of the camp refugees 65% were females while 35% were males. In total, 62.28% were married and had a mean age of 36 years old. The mean duration of their stay in the camp was 4.6 months.

Cohort medical profile and health services perceptions
In a scale from very good to very bad, 24.32% of females reported that their health condition were very bad, whereas only 7.69% of men reported the same. It is noteworthy that 59% of men characterized their health status as “bad/very bad” in contrast to 42% of women. Approximately 21% of women reported being in a good health status and 18% of men.
The majority of both men and women indicated that the main issue they encountered while they were staying in the camp was the nutrition problem. Particularly in men, 64.10% reported nutritional problems while in women 33.8% faced and treated it. Nutrition followed safety and hygiene problems. Specifically, safety was a particularly important for women (20%) while in men only 13%.
The main health problems that were reported by the subjects were chronic diseases medication and asthma for women with percentages that approximately reached 21% and 30% respectively as well as increased blood pressure (hypertension) in 30%. Men encountered similar problems with 41% of them being hypertensive. After their arrival in Jordan, people sought medical treatment after less than a month (mean 19 days), while 46% of them reported that they received “bad” services. This percentage in men was significantly increased (54%) compared to women (42%). 56% of people or a member of their family sought hospital care. During their stay in the camp, 55% of men felt anxious and 49% depressed, while 54% of both genders reported that the residency in the camp affected their health condition very much with 57% of them reporting that their health exacerbated during their stay. A significant proportion of people started smoking while in the camp (68%) with 78% of them were females.
Overall, 75% of people in the refugee camp argued that they received insufficient health care services. Additionally, 43% of people predicted that their health condition in future will significantly exacerbate, perhaps indicating the severity of health conditions of people in the camp.
Well- being of refugees
While at the camp, psychological and behavioural problems were improved. More specifically, 69% of people in the camp reported an attenuated melancholy problem, 52% of them reported an improvement in sleep while 64% reported increased confidence. Additionally, 52% reported no discrimination phenomenon during their stay in the camp. Communication with health provides or concern of not getting appropriate treatment did not pose significant problems. In fact, most refugees responded negatively regarding the existence of problems in accessing emergency medical or dentistry care with 42% and 50% respectively reporting absence of the problem of inaccessibility. Access to long term care though was a moderately serious problem for 20% of people. The vast majority of them didn’t encounter any hygiene problems, with 60% having access to clean water. Finally, refugees reported limited lack of help on behalf of the government and charity bodies (Table 3).
Multivariable analysis
We used an ordinal probit model to estimate the effect of each factor on the reported evaluation of health a 0.10 significance level (p<0.1) (Table 4).
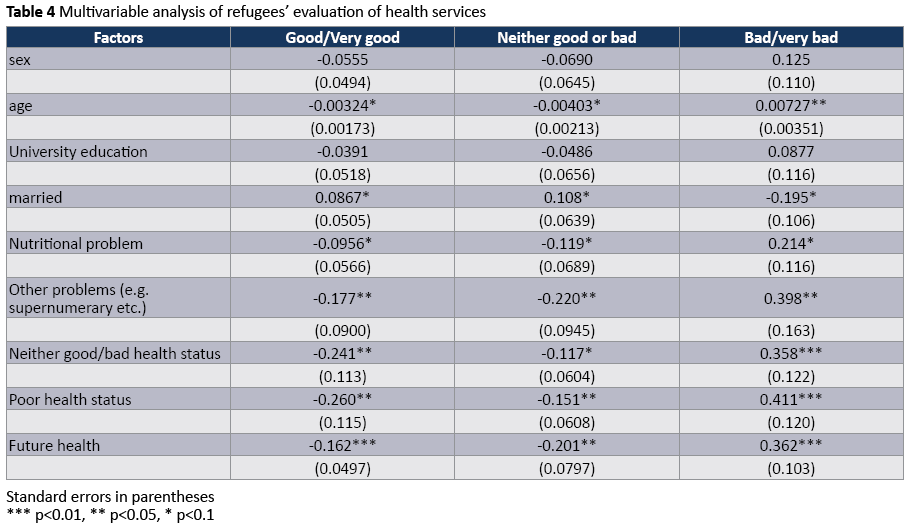
It is noteworthy that the probability of someone with poor health status to report an inadequate health service highly increases by 41.1 percentage points compared to someone that have a good health status. Finally, a strong association was found between a negative evaluation of health services and future projections of health status. Those who believed that would have an exacerbation in their health status increased their probability to report poor health services by 36.2 percentage points, while the probability of reporting positive health care services evaluation decreased by 16.2 percentage points. This is probably due to the fact that people expect their health to deteriorate since they received poor health services, or their expectation of having a low health status leads them to discredit the health services. Specifically, 68.47% of people believe that within the next 12 months, their health condition will exacerbate. Various health problems or discrimination feeling factor has no significant effect, hence they were omitted from the model.
Tobacco consumption and well-being
Smoking is an established risk factor for a range of clinical and psychological diseases, while several studies have highlighted its impact on subjective well-being [19,20]. More specifically, the majority of the available studies have reported negative correlations between smoking and life satisfaction or subjective well-being in selected subpopulations [21]. However, in our cohort, no significant association between smoking and psychological disorders was identified. This is potentially due to the limited sample size of our study. For a depressed person, the probability of being a non-smoker increases by 6.1 percentage points, while for an anxious person the probability increases by 5,7 percentage points (Table 5).

Discussion
As the crisis in Syria intensifies daily, with thousands continuing to flee to neighbouring countries to search for safety, humanitarian needs inside and outside the country are escalating rapidly [2]. Many patients have flooded into several hospitals in the countries around Syria. Within the Syrian Arab Republic, insecurity and the breakdown of the health system in many areas has substantially reduced access to health services. Health professionals, staff and patients continue to face difficulties reaching hospitals and health centers due to insecurity. Reports from November and December 2012 indicate that almost 55% of public hospitals, approximately 10% of health centers and 58% of ambulances have been damaged or destroyed. At least 31% of public hospitals are out?ofservice. There is also a severe shortage of medicines and medical supplies particularly for anaesthesia, surgical and trauma care, burn ointments, antibiotics, as well as supplies and equipment for treatment for cardiovascular disease, orthopaedic conditions and haemodialysis. The prolonged humanitarian situation has resulted in a growing unavailability of food, unhygienic and overcrowded living conditions, inaccessible or limited health care services and reduced immunization coverage for children under five. These combined factors increase the risk of communicable diseases and have serious implications on the nutritional status of children under five and pregnant and lactating women.
On the other hand, the last decade Jordan has accommodated a lot of people, Palestinian, Iraqi, Libyans and now Syrian. Jordan has not signed the Geneva Convention on the Status of Refugees, and refugees in Jordan are considered ‘guests’, ‘not acknowledged as refugees for whom the state takes responsibility [22]. Jordan has an advanced health care system. The total expenditure on health as % of GDP in 2011 was 8,4%. Jordan is ranked by the World Bank to be the number one health care services provider in Middle East and among the best in the world. Jordan has emphasized in education, health, water, sanitation and hygiene and SGBV and child protection services. The Government of Jordan has allowed to Syrian people full access to health care services not only in Primary Health Care but in hospitals too [23,24]. These people enjoy the same services as the Jordanian population. Services are overemphasized. Infectious disease epidemics until now are in very low levels, but effort should be continued otherwise Jordan’s health sector will suffer corrosion on what they have achieved the last years [25]. Mental health services have been supported in five clinics in four geographical areas, primarily for Syrian patients in Irbid, Mafraq, Ramtha and Amman including MH services in Zaatri camp. 783 consultations have been made to 220 mental health patients. Since 1 January, 111,205 Syrian children have been reached by psychosocial support services. Mental health services are provided by military hospitals too [21].
Lack of awareness and access to mental health patients in urban settings and the fear of stigmatization are the main mental health challenges. Between March and October 25,482 Syrians accessed primary health care services at UNHCR supported clinics with 4,507 being under aged five.
One cannot ignore the high economic costs to the Jordanian government for health services, and the indifference of the international community (with minor exceptions) for assistance. Zaatri camp costs $500.000 a day to run, according ECHO. In fact, the amount is not sufficient. Only EU doubled their help to the Hashemite Kingdom to €226m. Antoine Foucher, {head of mission for Médecins Sans Frontières (MSF) in Jordan} declared that “Without political will and financial commitment from global community, the Jordanian government risks resorting to drastic measures: permanently blocking refugee access to the country or restricting access to care in public facilities, undermining the already precarious living conditions of hundreds of thousands of Syrians,” [26].
In spite of Jordan facing its own challenge (hard economic times) Syrian refugees have been welcomed by Jordanian government (showing tolerance and hospitality) and many local communities continue to extend hospitality and assistance in spite of their own often limited means [20]. The borders remain opened and the protection space offered Syrians has not shrunk at any time. 70 per cent of Syrian refugees in Jordan live amongst host communities, with the rest accommodated in three camps. Zaateri the largest camp is estimated to have more than 120.000 people.
International Organization for Migration has screened to date 36,545 newly arriving Syrians over the age of 15 for TB and have detected 14 TB cases of which 3 are extra pulmonary. 32,760 people have been reached with TB awareness sessions. TB is a very severe disease and prevention measures must be taken. The Moroccan military field Hospital in Zaatri since August has provided over 52,000 consultations, over 83,000 services, 152 surgeries, conducted 46 deliveries including 20 caesareans sections. Over 124,000 children has obtained supplies and supported immunization. Due to the high percentage of chronic or non-communicable diseases such as diabetes, hypertension, ischaemic heart diseases and cancers to manage all these is too costly and complex for Jordanian health sector. From 1 to 21 November National Immunization Campaign vaccinated 3.29 million people against measles (99% of target) and 1.1 million children against polio (120% of target). 671,527 children received vitamin A (67% of target). Some 106,733 Syrian children are now enrolled in schools in Jordan, including 20,990 in camp schools. In general, Jordanian Ministry of Health has spent 53 million US $ for four months between January and April 2013 [8,27-29].
In the meantime, the crisis in Syria is continuing to evolve and the steady influx of refugees in Jordan is constantly growing [30]. Jordanian government estimates that more than 1.2 million Syrian people live currently in Jordan. Of them more than 80% are not living in the four camps that are available [31]. Approximately 3/4 of those people report that the provided health services are insufficient. This is apparent since a large percentage (59% of men and 42% of women), characterize their health status as bad and very bad. Evidently, 46% of the population reports bad health services reception. However, the most concerning issue is that these services were received after 3 weeks stay in the camp. Additionally, of primordial importance for health services provided to this population is that 57% report that the state of their health deteriorated during their stay in the camp. However we should take into account that the number of immigrants is large, and a great part of them requires health services.
Generally, regarding psychological problems, confidence issues and melancholy, immigrants reported significant improvement. This may be due to security feelings that the camp might offer to them and their families. It is noteworthy that the majority of the Syrians believe that psychological problems can lead to stigmatization. Syria Bright Future (SBF) a non-political Syrian organization in Jordan, reported that in the few months that they have been working in Jordan, the psychologist and the whole team, have helped almost 100 patient with mental problems, and more than 200 injured people that should urgently see a specialist. From those, 45 ultimately required specialized care [21].
According to Rochelle and Taylor some Syrian refugees in Jordan, people in the camps feel extremely safe and secure, and are grateful to the Jordan population and government. In contrast to them, Somalian and Sudan refugees feel hopeless and neglected. The health care services (primary, secondary and tertiary) provided to the registered Syrian people in Jordan are free. Regarding the non-registered population, it has free primary health care services and secondary and tertiary health services from international and national NGO providers, as well as international and local charitable organizations [19].
Regarding the Jordanian population, according to a study conducted by the University of Jordan's Centre for Strategic Studies, 70% of Jordanians demand from their government to forbid more Syrians to cross the border and take up residence in Jordan. 75% of population argues that the Jordanian government should make a buffer zone within Syria to host refugees and this zone to be commanded by United Nations [32]. A major problem for them is that 58% of the population believes that due to the refugees, the public services provided to the Jordanian citizens have been heavily reduced [33]. Despite this, hospitability of Jordanian people and Jordanian government must be recognized. Jordan has long history of hosting refugees and responding to crises. We must emphasize that the country has prevented a wide scale humanity disaster by keeping their borders open, which has come at considerable cost to its population and budget.
Conclusions
The provision of health services to Syrian refugees in Jordan is in fairly good level. This is shown by the survey results, although in some cases there are several weaknesses and problems that certainly need to be addressed. One of the most positive is the safety that these people feel to their new place of residence.
However, the challenges are enough and can only be solved with the international community help. The international community apart from providing financial assistance, should also provide medicines and specialized health personnel [34].
As for the country itself, it has been created a huge economic problem on which the Kingdom is trying to deal with austerity measures. But, this has the effect of lowering the quality of health services in their own county’s citizen.
Conflict of Interest
No con?icts of interest have been reported by the authors or by any individuals in control of the content of this article.
Funding
No funding was received in order to conduct this study.
Ethical Approval
It wasn’t necessary to take a written concerned from each participant at the survey. All ethical issues have been taken into consideration since doctor Amjed Al-Fahoum who is Director of the Excellence center at Yarmouk University in Irbid (Jordan) informed us about the ethical issues existing in Jordania and the ways to respect them. Additionally, we have taken an oral informed consent from each participant who voluntarily accept to participate in the survey without any acquistion and coercion. Questionnaires were administered by a native speaker of the Arabic language, so no language barriers interfered with communication, something that helped us more to recognize and respect all the excisting ethical issues.
5185
References
- Selm JV (2005) European Refugee Policy: Is There Such a Thing? NewIssues in Refugee Research, Working Paper No. 115. Migration PolicyInstitute, Washington DC, USA.
- Owen P (2013) Syria refugee crisis – a day in the life. The Guardian www.unrefugees.org/site/c.lfIQKSOwFqG/b.4950731/
- El-Khatib Z, Scales D, Vearey J, Forsberg B (2013) Syrian refugees, between rocky crisis in Syria and hard inaccessibility to healthcare services in Lebanon and Jordan. Confl Health 7: 18.
- WHO (2013) Health response to the crisis in the Syrian Arab Republic and neighboring countries.
- UNHCR (2013) Inter-Agency Regional Response For Syrian Refugees Egypt, Iraq, Jordan, Lebanon, Turkey 12 - 18 September 2013.
- Murshidi M, Hijjawi M, Jeriesat S, Eltom A (2013) Syrian refugees and Jordan’s health sector. Lancet 382: 206–207.
- UNHCR (2013) Syrian Refugees at a Glance Egypt, Iraq, Jordan, Lebanon and Turkey. February 2013. UN High Commissioner for Refugees.
- UNHCR (2013) All statistics on refugees are from “Demographic Data of Registered Population,” Syria Regional Refugee Response Information Sharing Portal. UN Refugee Policy, Turkey.
- Huber M, Stanciole A, Bremner J, Wahlbeck K (2008) Quality in and Equality of Access to Healthcare Services. European Commission, Brussels.
- Lacroix M (2006) Social work with asylum seekers in Canada: the case for social justice. Int Soc Work 49: 19-28.
- Lavenex S (2001) The Europeanization of refugee policies: normative challenges and institutional legacies. J Common Mark Stud 39: 851-874.
- Watters C (2002) Migration and mental health care in Europe: report of a preliminary mapping exercise. J Ethn Migr Stud 28: 153-172.
- National Association of Countries (2010) Immigration focus questionnaire.
- Abe-Kim J, Takeuchi DT, Hong S, Zane N, Sue S, et al. (2007) Use of mental health-related services among immigrant and US-born Asian
- Americans: Results from the National Latinoand Asian American Study. Am J Public Health 97: 91−98.
- Cheng EM, Chen A, Cunningham W (2007) Primary language and receipt of recommended health care among Hispanics in the United States. J Gen Intern Med 22: 283−288.
- Institute of Medical Anthropology (2008) Health Care Related Issues in Latin American Immigrants in Saitama and Gunma. Waseda University, Tokyo.
- Rosewich M, Schulze J, Eickmeier O, Adler S, Rose MA, et al. (2012) Early impact of smoking on lung function, health, and well-being in adolescents. Pediatr Pulmonol 47: 692-699.
- McCann SJH (2010) Subjective well-being, personality, demographic variables, and american state differences in smoking prevalence. Nicotine Tob Res 12: 895-904.
- Kasapoglu, A, Ozerkmen N (2008) Predictors of adolescent cigarette smoking behavior: A sociological case study in Ankara, Turkey. J Child Adoles Subst Abuse 17: 115–132.
- Lacroix M, Al-Qdah T (2012) Iraqi refugees in Jordan: Lessons for practice with refugees internationally Eur J Soc Work 15: 223-239.
- Roberts I (2013) Syrian refugees and Jordan’s health sector. The Lancet 382.
- El Farouki G (2013) Jordan’s health care system. The Jordan Times, Jordan.
- WHO (2006) Health System Profile-Jordan. Regional Health Systems Observatory – EMRO.
- https://www.ourmediaourselves.com/archives/111pdf/Syrian_ mental_health_professionals_as_refugees_in.8.pdf
- UNICEF (2013) Syria crisis. Bi-weekly humanitarian situation report. 15-28 November: Syria, Jordan, Lebanon, Iraq, Turkey and Egypt.
- UNHCR (2013) Syrian Refugees at a Glance Egypt, Iraq, Jordan, Lebanon and Turkey.
- Tisdall S (2014) Inside a refugee camp in Jordan three years after the Syrian uprising began. The Gurdian.
- Rochelle D, Taylor A (2013) Syrian Refugees in Jordan and Lebanon: A Snapshot from Summer 2013. The Center for Contemporary Arab Studies, The Institute for the Study of International Migration.
- https://jordantimes.com/majority-of-jordanians-call-for-end-to-syrian-refugee-influx accessed Feb. 2014
- Doedens W, Giga N, Krause S, Onyango MA, Sami S, et al (2013) Reproductive Health Services for Syrian Refugees in Zaatri Refugee Camp and Irbid City, Jordan. Boston University, USA.
- https://www.msf.org/article243/syrian-refugees-jordan-limits-assistance

