Keywords
Nurse, education, cardiac event, coronary artery bypass graft, rehabilitation.
Introduction
During recent decades, the role of cardiac rehabilitation has been the focus of attention by the vast majority of literature. Effective rehabilitation is a multifactorial intervention requiring involvement of many health professionals with nurse to be in the front line [1-4].
The main goal of cardiac rehabilitation is to prompt patients participate in their therapeutic treatment regimen to such an extent that they can achieve living almost a normal life. Cardiac rehabilitation programs comprising prescriptive exercise, health education, and counseling, yield compelling improvements in cardiac morbidity and mortality of participants [5,6]. Furthermore, detection, diagnosis and monitoring of psychological distress should be part of rehabilitation since after admission patients frequently experience clinically significantly levels of anxiety or depression that may persist for long thus affecting the outcome of cardiac disease. Usually, health professionals fail to recognize psychological distress in patients with coronary artery disease because they perceive it as a normal reaction to the stressful event of acute myocardial infarction. As a result, symptoms are misdiagnosed as physical problems while the underlying cause remains [7,8].
Education provided in rehabilitation should be individualized according to the patients' needs and personal beliefs or attitudes. For instance, though patients with coronary disease of similar demographic and socio-economic characteristics may have common healthcare needs, however there are also specific needs unique to each patient group, attributable to the impact of coronary artery disease [9].
The significant role of integrating education in a rehabilitation programme has been widely acknowledged by all health professionals. Education is the process of acquiring knowledge and skills that can lead to changes in human behavior, necessary for the maintenance or improvement of health. More in detail, to achieve optimal benefit for patients, education should involve definition of goals, assessment of patients' needs, modification of patient’s behavior towards more self-control, active participation n decision making, development of self-care to handle the disease and possible complications, assessment of personal risk factors, implementation of realistic goals, support to adopt a positive attitude towards the disease and alleviate psychological distress. The learning process (ways of learning, duration of sessions) differs among individuals, and depends mainly on the apprehension of participants and their personal goals [10,11-15].
Education that focuses on the patient is associated with increased patient satisfaction, lower levels of anxiety and depression, high levels of compliance to treatment, as well as improved quality of life not only for the patients but for their supporting environment [10,11-15].
Though education has an essential role in patients' rehabilitation, however its' value is under-recognized in daily clinically practice owing to many reasons such as non availability of spare time and staff personnel or to the fact that more emphasis is put on the treatment of the disease [7]. Given the fact that hospital stay is minimizing, neither health professionals nor patients have adequate time to devote to their education [8]. Consequently, education should start immediately after the diagnosis of the disease [11-15].
On the other hand, education of health professionals is a prerequisite of an effective treatment. Apart from theory knowledge, they need to improve their skills regarding knowledge transmission, ability to help patients express their feelings thus following educational programmes [11-15]. Furthermore, health professionals, fail to recognize psychological distress due to their lack of education on the typical and atypical symptoms [8].
The aim of this review was to present the role of nursing education in cardiac patients’ outcome.
Material and Method
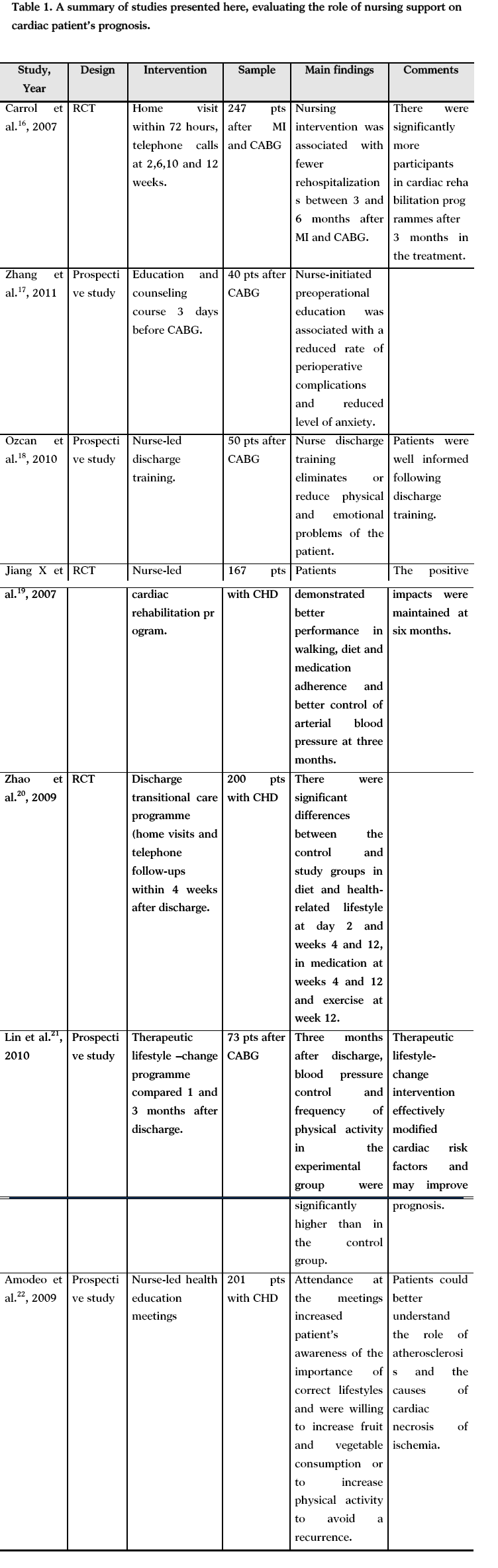
Studies published in English between 2002 and 2011 were selected through a computer-assisted literature search (i.e., Pubmed https://igm.nlm.nih.gov, and Scopus www.scopus.com). The computer searches used combinations of Keywords relating to the role of nursing (i.e., nursing support, nursing training, nursing education, coronary artery disease) and cardiac rehabilitation. In addition, the reference lists of the retrieved articles helped us to find relevant to the present articles that did not allocate through the searching procedure. The following information (when available) was presented according to a fixed protocol: design of study (i.e., observational study, clinical trial), sample size, mean age and sex of participants, follow-up duration and degree of adjustment for potential confounders. Thus, 15 studies were selected and discussed; of them 4 were prospective, 4 were clinical trials and 7 were reviews, (Table 1).
The role of nursing education
Some studies [16,17] have revealed the value of nursing practice in secondary prevention and disease management. Cardiac rehabilitation programs including nursing education exert a beneficial effect on patients' quality of life, exercise capacity, lipid profile, body mass index, body weight, blood pressure, resting heart rate, survival rate, mortality rate and decreased myocardial infarction risk factors.
Given the fact that the role of nurses in providing education is multidimensional Riccio et al., [18] demonstrated that this role may be categorized in three different levels: a) technical level needed to carry out diagnostic tests and based on cooperation with cardiologists, b) a second level at which nurses provide information to patients and in-hospital counseling so as to help them combat the disease and be actively involved in the medical treatment, and c) providing psychological support both to the patient and the family during acute illnesses about the treatment.
It is widely accepted that the period during hospitalization is considered the most appropriate for starting rehabilitation and identify those patients who are in need of intense and elaborate treatment. Accordingly, follow-up programs conducted by well trained in cardiology and cardiovascular prevention professional nurses are of vital importance.
However, after discharge of hospital many reasons are held responsible for participation in rehabilitation. Carroll et al., [19] made an effort to determine if nurse intervention increase participation in cardiac rehabilitation programmes thus reducing hospital readmission after MI and coronary artery bypass graft surgery, (CABG). This trial enrolled 247 patients. Subjects were randomized into 4 groups: standard of care group for MI and for CABG and standard of care plus the treatment groups for MI and for CABG, for 12 weeks after discharge. The treatment consisted of a community-based intervention of a home visit within 72 hours and telephone calls at 2, 6 and 10 weeks from an advanced practice nurse and 12 weekly telephone calls from a peer advisor. Participation in a cardiac rehabilitation programme and rehospitalizations were collected at 6 weeks and 3, 6 and 12 months by telephone interview. There were significantly more participants in cardiac rehabilitation programmes after 3 months in the treatment group, and this increase was seen up to 1 year after MI and CABS. There were no statistical differences, although there were fewer rehospitalizations between 3 and 6 months after MI and CABG in the treatment group compared with the standard of care group. Overall, the evidence from this study suggests that a community based collaborative peer advisor/advanced practice nurse intervention can play a role in promoting active participation in cardiac rehabilitation programmes.
Education provided at discharge following open heart surgery increases the knowledge of patients according to the study conducted by Ozcan et al. [20] Indeed, education training after open heart surgery is beneficial as it eliminates or reduces physical and emotional problems of the patient.
The important role of nurse is not limited in interventions after cardiac event but also is equally significant in pre-operative stage as demonstrated by Zhang et al., [21] who explored the effect of nurse-initiated preoperative education and counseling on postoperative complications and anxiety symptoms following CABG. The studied sample included 40 patients who were divided into the study and control groups. All patients received standard preoperative and postoperative care, but the study group patients also completed a structured education and counseling course supervised by designated nurses 3 days before the surgery. The conclusion that stems from this study is that nurse-initiated preoperational education and counseling were associated with a reduced rate of perioperative complications and a reduced level of anxiety following CABG. According to the results of study conducted by Jiang et al., [22] a nurse educational programme can significantly improve the health behaviors and cardiac physiological risk parameters in coronary heart disease patients. The studied sample (n = 167) were randomly assigned to either an intervention group (the cardiac rehabilitation program) or control group (the routine care). The change of health behaviors (walking performance, diet adherence, medication adherence, smoking cessation) and physiological risk parameters (serum lipids, blood pressure, body weight) were assessed to evaluate the program effect. Patients in the intervention group demonstrated a significantly better performance in walking, diet adherence, medication adherence; a significantly greater reduction in serum lipids including triglyceride, total cholesterol, low-density lipoprotein; and significantly better control of systolic and diastolic blood pressure at three months. The majority of these positive impacts were maintained at six months. Nurses can fill significant treatment gaps in the risk factor management of patients with coronary heart disease.
Zhao et al., [23] in a randomized controlled trial explored the effects of a postdischarge transitional programme among patients with coronary heart disease. The research included 200 patients; the control group (n = 100) received routine care and the study group (n = 100) received the postdischarge transitional care program, which consisted of predischarge assessment, structured home visits and telephone follow-ups within four weeks after discharge. There were significant differences between the control and study groups in diet and health-related lifestyle at day 2 and weeks 4 and 12, in medication at weeks 4 and 12 and exercise at week 12. The results of this study showed the effectiveness of the program indicating that such programmes help patients maintain a healthy lifestyle and thereby control the risk factors.
The behavioral and clinical impact of a therapeutic lifestyle-change intervention for cardiac risk factors in patients after CABG was also demonstrated by Lin et al., [24] who enrolled in their study 73 patients. The control group (n = 37) and experimental group (n = 36) both received routine postoperative rehabilitation, with the experimental group also receiving the therapeutic lifestyle-change program. Measures of behavioral and clinical outcomes were compared before surgery, 1 and 3 months after discharge. The results revealed that the amount of cigarette smoking, blood pressure control, frequency of physical activity and dietary behavior were modified in both groups to the first month. Three months after discharge, blood pressure control and frequency of physical activity in the experimental group were significantly higher than in the control group. In conclusion, the therapeutic lifestyle-change intervention into a rehabilitation program effectively modifies cardiac risk factors and may improve postoperative recovery and prognosis.
The importance of educational intervention for patients with coronary artery disease led by nurses involving regular health education meetings for patients and their relatives has been also underlined by Amodeo et al. [25] 201 patients attended a meeting, where cardiac risk factors and prevention of recurrences, were discussed. Attendance at the meeting significantly increased patients’ understanding of atherosclerosis and the causes of cardiac necrosis or ischemia. The meeting enhanced awareness about modification of lifestyle and prompt patients’ willingness to increase fruit and vegetable consumption or to increase physical activity.
On contrary, other studies [26-28] support that the contribution of nurses to risk factor management and their educational strategies are minimal and weak compared to that of other caregivers. It is cited that there are obstacles (lack of nursing staff, absence of communication with nurses, cost management problems) which hamper development of cardiac rehabilitation services.
Providing an effective, safe, individualized and culturally adjusted rehabilitation programmes for patients after a cardiac event is a matter of great priority for each Health System. In that way, these programmes can reduce subsequent mortality and help people understand the future risks [29,30].
Undoubtedly, nurses are the only health professionals who attend patients from admission to hospital until discharge, thus having an overall perspective of patient’s problems and needs [16].
However, extensive argument is noted in the literature about the source, the type and extent of information or education provided patients with coronary artery disease. The source of education either by medical or nursing staff has been controversial since it is not completely understood whether nurses as an interdisciplinary team are the best. Professionalism of physicians and nurses and the politics of hospital organization (private or public) exert a decisive role on the quality of education [31].
Conclusion
Nurses represent a large proportion of health care community. They play a vital role in treatment as they are close to the patients and their families during all the process of disease. It is a matter of great importance for nurses to meet the rehabilitative care needs of patients through education, support, supervision and reinforcement.
Nursing education in cardiac rehabilitation can improve health outcomes and reduce the risk of a new cardiac event. A health educational programme organized by nurses for patients after a cardiac event or surgery improves patients’ knowledge of their illness and awareness of behavioral changes to prevent a new event or readmission to hospital.
3153
References
- Cohen C. Rehabilitation nursing: thoughts on a specific role. Rev Med Suisse Romande. 2001 ;121(6):417-21.
- Fridlund B. The role of the nurse in cardiac rehabilitation programmes.Eur J CardiovascNurs. 2002 ;1(1):15-8.
- Long AF, Kneafsey R, Ryan J, Berry J.The role of the nurse within the multi-professional rehabilitation team.JAdvNurs. 2002;37(1):70-8.
- Long AF, Kneafsey R, Ryan J.Rehabilitation practice: challenges to effective team working. Int J Nurs Stud. 2003;40(6):663-73.
- BeckieTh, Beckstead J. Predicting Cardiac Rehabilitation Attendance In A Gender-tailored Randomized Clinical Trial J CardiopulmRehabil Prev. 2010 M; 30(3): 147–156.
- Antúnez de la Rosa Mdel R, Jiménez y Villegas Mdel C. Nurses' participation in heart rehabilitation. Arch Cardiol Mex. 2002;72Suppl 1:S247-53.
- Amin A, Jones A, Nugent K, Rumsfeld J, Spertus J. The prevalence of unrecognized depression in patients with acute coronary artery disease. Am Heart J. 2006;152(5):928-934.
- Polikandrioti M. Needs of depressed patients with coronary artery disease. Health Science journal. 2011;5(4):241-242.
- Asadi-Lari M, Packham C, Cray D. Psychometric properties of new health needs analysis tool designed for cardiac patients. Public Health. 2005;119(7):590-98.
- Polikandrioti M, Νtokou M. Needs of hospitalized patients. Health science journal. 2011;5(1):15-22.
- Nolan J, Nolan M, Booth A. Developing the nurse's role in patient education: rehabilitation as a case example. Int J Nurs Stud. 2001;38(2):163-73.
- Smith J, Liles C. Information needs before hospital discharge of myocardial infarction patients: a comparative, descriptive study. J ClinNurs. 2007;16(4):662-71.
- Lanuza DM, Davidson PM, Dunbar SB, Hughes S, De Geest S. Preparing nurses for leadership roles in cardiovascular disease prevention. J CardiovascNurs. 2011;26(4 Suppl):S56-63.
- McPherson CP, Swenson KK, Pine DA, Leimer L.A nurse-based pilot program to reduce cardiovascular risk factors in a primary care setting. Am J Manag Care. 2002;8(6):543-55.
- Cao Y, Davidson PM, DiGiacomo M. Cardiovascular disease in China:an urgent need to enhance the nursing role to improve healthoutcomes. J ClinNurs. 2009;18(5):687-93.
- Cynthia D. Nurse practitioner role in cardiac rehabilitation enhances adherence to evidence-based guidelines. Journal of Cardiopulmonary Rehabilitation & Prevention. 2006;26(4):255-255.
- Eshah NF, Bond AE. Cardiac rehabilitation programme for coronary heart disease patients: an integrative literature review. Int J NursPract. 2009;15(3):131-9.
- Riccio C, Sommaruga M, Vaghi P, Cassella A, Celardo S, Cocco E, et al. Nursing role in cardiac prevention. Monaldi Arch Chest Dis. 2004;62(2):105-13.
- Carroll DL, Rankin SH, Cooper BA. The effects of a collaborative peer advisor/advanced practice nurse intervention: cardiac rehabilitation participation and rehospitalization in older adults after a cardiac event. J CardiovascNurs. 2007;22(4):313-9.
- Ozcan H, YildizFindik U, Sut N. Information level of patients in discharge training givenby nurses following open heart surgery. Int J NursPract. 2010;16(3):289-94.
- Zhang CY, Jiang Y, Yin QY, Chen FJ, Ma LL, Wang LX. Impact of Nurse-Initiated Preoperative Education on Postoperative Anxiety Symptoms and Complications After Coronary Artery Bypass Grafting. J CardiovascNurs. 2011; 46(2):198-202.
- Jiang X, Sit JW, Wong TK. A nurse-led cardiac rehabilitation programme improves health behaviours and cardiac physiological risk parameters: evidence from Chengdu, China. J ClinNurs. 2007;16(10):1886-97.
- Zhao Y, Wong FK.Effects of a postdischarge transitional care programme for patients with coronary heart disease in China: a randomised controlled trial. J ClinNurs. 2009;18(17):2444-55.
- Lin HH, Tsai YF, Lin PJ, Tsay PK. Effects of a therapeutic lifestyle-change programme on cardiac risk factors after coronary artery bypass graft. J ClinNurs. 2010;19(1-2):60-8.
- Amodeo R, De Ponti A, Sorbara L, Avanzini F, Di Giulio P, De Martini M. How to increase patient knowledge of their coronary heart disease: impact of an educational meeting led by nurses.GItalCardiol (Rome). 2009;10(4):249-55.
- Scholte op Reimer WJ, Jansen CH, de Swart EA, Boersma E, Simoons ML, Deckers JW. Contribution of nursing to risk factor management as perceived by patients with established coronary heart disease. Eur J CardiovascNurs. 2002;1(2):87-94.
- Wang W, Chair SY, Thompson DR, Twinn SF. Health care professionals' perceptions of hospital-based cardiac rehabilitation in mainland China: an exploratory study. J ClinNurs. 2009;18(24):3401-8.
- Tod AM, Lacey EA, McNeill F. 'I'm still waiting...': barriers to accessing cardiac rehabilitation services. J AdvNurs. 2002;40(4):421-31.
- Beswick AD, Rees K, Griebsch I, Taylor FC, Burke M, West RR, et al. Provision, uptake and cost of cardiac rehabilitation programmes: improving services to under-represented groups. Health Technol Assess. 2004;8(41):1-152.
- Marvaki C, Argyriou G, Karkouli G, Kossivas P, Marvaki A, Pilatis N, et al. The role of education on behavioral changes to modifiable risks factors after myocardial infarction. Health Science Journal. 2007; 1(3):1-8.
- Moret L, Rochedreux A, Chevalier St, Lombrail P, Gasquet I. Medical information delivered to patients: Discrepancies concerning roles as perceived by physicians and nurses set against patient satisfaction. Patient Education and Counseling, 2008;70(1):94-101.

