Key words
Emergency Department, polytrauma patient, time-to-treatment, Emergency Department Length of Stay (ED LOS), Injury Severity Score (ISS)
Introduction
Emergency Department (ED) is the place of a hospital where emergency cases are admitted, checked and managed. Acute myocardial infraction, cardiopulmonary arrest, allergic shock, stroke, asthma and status epilepticus are included in emergency cases. Polytrauma patient is considered to be an identical case too. [1]
The mission of emergency departments is to provide emergency medical services and ensure survival for patients with urgent health problems. Initial management and diagnosis of polytrauma patients is provided in the ED. [2-4]
Every patient having multiple trauma, which is equal with multiple critical injuries on different anatomical areas of the body, or having Injury Severity Score (ISS)>15, is considered to be polytrauma patient. [5] ISS is an international scale of describing, categorizing and estimating the severity of polytrauma patient’s injuries. Such scale is Revised Trauma Score (RTS) too. [6,7]
The time needed for a trauma patient’s primary and secondary evaluation and management in the ED is called time-to-treatment and is equal with the patient’s ED length of stay (ED LOS). During primary evaluation trauma patient is checked according to the algorithm ABCDE and during the secondary trauma surgeon examines patient during anatomical areas and asks the necessary diagnostic tests.
Time-to-treatment begins with polytrauma patient’s admission in the ED and ends by the time patient has been diagnosed and transported to the appropriate department for further treatment. [8] This time interval is usually affected by saturation and increased traffic of the ED. [9]
The American College of Surgeons suggests that «golden hour» is the ideal time for evaluation and management of polytrauma patient. [10] Golden hour represents the first 60 minutes from the moment of injury and the golden hour theory is basic principle in Emergency Medical Care providers. [11-15] After all, for several decades rapid intervention is believed to improve final outcome of trauma patients, which is very important since trauma is considered to be the first cause of death worldwide for people aged from 0 to 40 years old. [16]
Purpose
The aim of the present study was to estimate polytrauma patients’ time-to-treatment in the ED.
Material and Method
The sample population of the present study consisted of 53 polytrauma patients aged over 14 years old with Injury Severity Score (ISS)>15 who were transported to the ED of a general hospital in Athens and having complete the whole diagnostic procedure in the ED. Data collection took place between June of 2010 and February of 2011. Time-to-treatment begun with polytrauma patient’s admission in the ED and fulfilled with patient’s transportation to the appropriate department for further treatment.
Demographic characteristics, time intervals for transportation and initial treatment, vital signs, Glasgow Coma Scale (GCS), types of injuries, diagnostic tests and ED LOS for each patient were recorded in a special registration form. The severity of injuries was evaluated with ISS and Revised Trauma Score (RTS) and the days of hospitalization were calculated. The registration form was developed by the researchers for this study and the use of it took place under permission of the Scientific Committee of the hospital in which the research was conducted. All rules have been complied with ethics.
Statistical Analysis
The statistical analysis was performed by SPSS for Windows (Version 17) and multiple linear regression, logistic regression and Spearman’s Rho correlation coefficient were used as tests.
To find the correlation between quantitative variables and polytrauma patients’ ED LOS Spearmans’ Rho criterion was used. Multiple linear regression analysis was applied to compare the impact of the explanatory variables to polytrauma patients’ ED LOS. To find the correlation between severity variables (age, SpO2, SAP, ISS, RTS and ED LOS) and patients’ outcome (survival or death) univariate logistic regression analysis was applied and factors having p>0.01 were excluded. Factors having p≤0.01 were edited with multiple logistic regression analysis and those having p <0.05 were assessed. The statistical significance was p<0.05.
Results
Descriptive
The sample studied consisted of 53 polytrauma patients; 81.1% (n=43) were men. 75.5% (n=40) were Greek people and the rest were foreigners. The mean age of the study participants was 43±20 years and the severity of injuries was according to ISS 23±8 and RTS 7.38±1. Regarding the cause of injury, 17% (n=9) of the sample had a fall from height, 18.9% (n=10) was entrainment by a moving vehicle, 34% (n=18) had motorcycle accident and 15.1% (n=8) had a car accident. According to the results of the study 9.4% (n=5) of patients involved in a motorcycle or car accident had a helmet or a safety belt on. Moreover, 15.1% (n=8) of patients had extensive burns (2 cases), beating injuries (5 cases) and electrocution followed by fall from height (1 case). The mean transportation time to the ED was 59±41 min. When patients admitted to the ED their heart rate (HR) was 101±22 bpm, their O2 saturation(SpO2) was 93±7% with respiratory rate (RR) 29±6/ min and their Mean Arterial Pressure (MAP) was 88±20 mmHg with Systolic Arterial Pressure (SAP) 123±30 mm Hg. Study population’s level of consciousness was estimated according to GCS and their score was 13±3. The diagnostic tests used to evaluate patient’s condition were: abdominal ultra sound examination (u/s) and x-rays for 66% (n=35) of the sample. The time needed to complete the above examinations was 40±17 min in radiology department. A whole body Computed Tomography scan (CT whole body) was used for 47.2% (n=25) of the participants, 18.8% (n=10) of the sample had no CT scan, while the remaining 33.9% (n=18) had a focused CT scan on selected anatomical regions of their body. Time consumed in the CT department for patients’ examination was 35±20 min. The total time needed for all imaginary studies (u/s, CT, x-rays) for patients was 68±27 min. Regarding the interventional medical procedures: 17% (n=9) of the sample were intubated either in ED or during admission, 20.8% (n=11) had a central venus line (CVL), while 1.9% (n=1) had a pleur evac, 18.9% (n=10) of the studied population had a nasogastric tube and 67.9% (n=36) had an urine catheter. Suturing of lacerations was performed in 35.8% (n=19) of patients. The complete diagnostic control of polytrauma patients usually included examinations by chest surgeons, neurosurgeons, maxillofacial surgeons and orthopaedic surgeons. Rarely a plastic surgeon, ophalmologist and urologist were needed. The time consumed for patients’ examinations by all necessary specialists was 121±100 min. The total ED LOS of polytrauma patients was estimated to be 372±232 min. After their stay in ED, 13.2% (n=7) of patients were admitted in a clinical department of the hospital, 54.7% (n=29) were admitted in intensive care unit (ICU), 30.2% (n=16) were transferred to the operating room in an emergency basis and 1.9% (n=1) died during their management in ED. The final outcome of patients was: death, for 18.9% (n=10) during their hospital stay and discharge, for 81.1% (n=43) of the sample studied.
Statistics
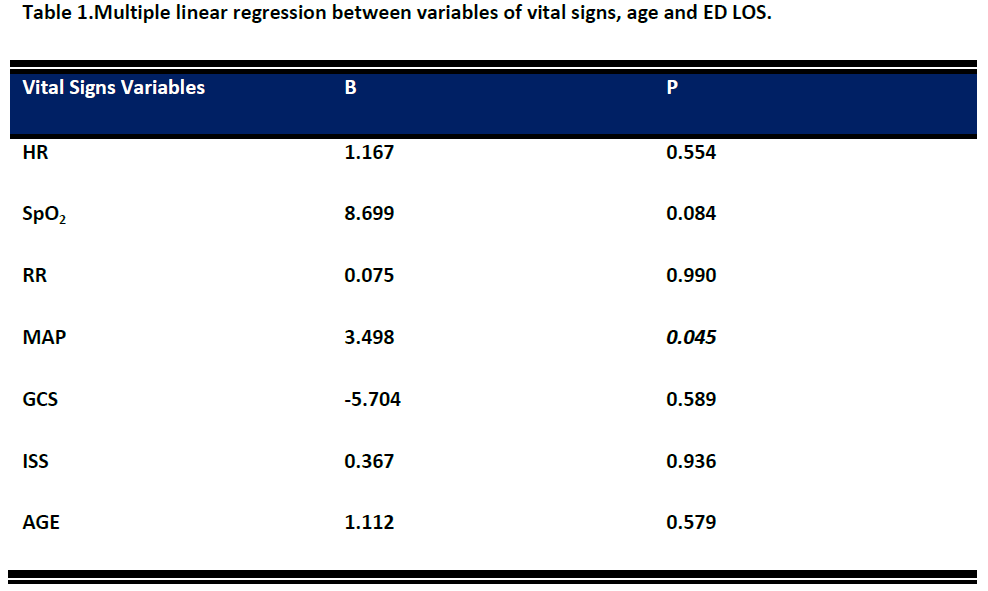
By applying linear regression analysis, it was revealed that where the ED LOS was examined in relation with all the indicators of vital signs (VS), patients’ ED LOS was affected marginally by MAP (p=0.045). Specifically, it was revealed that for every increasing unit of MAP of patients, ED LOS was increased 3.5 times (Table 1). Additionally, with the same method of linear regression analysis, by modifying the variables that represent:
• The number of medical specialists that should examine patients and the necessary time for their examination,
• The number of necessary x-rays for patients’ diagnosis and the time needed for them along with the abdominal u/s,
• The time needed for the completion of CT scan requested for each patient and
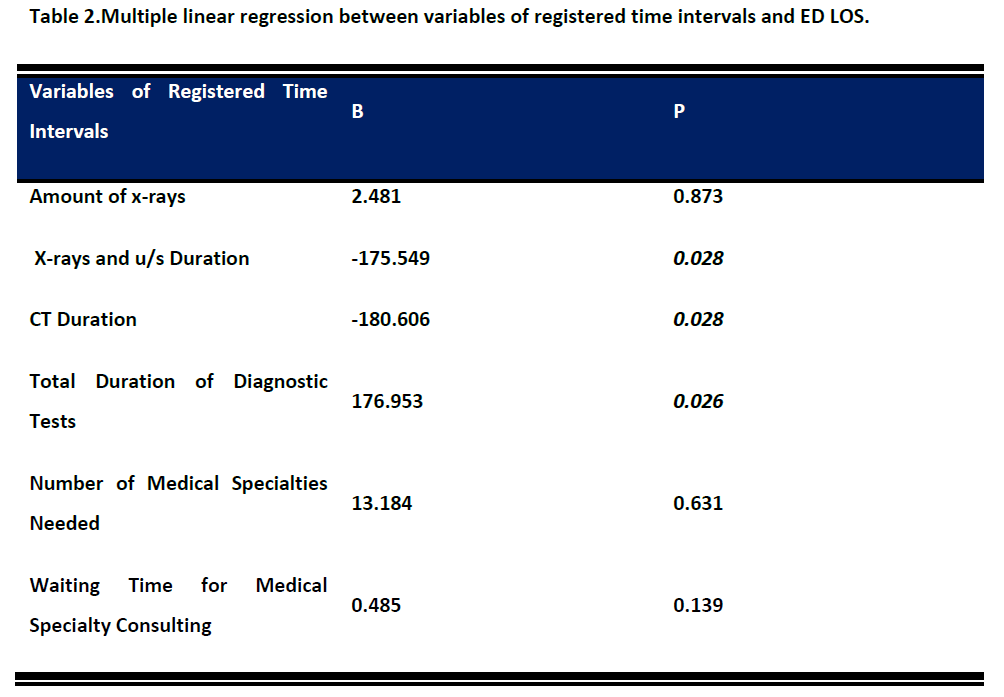
• The total duration of diagnostic examinations carried out in ED for each patient it was concluded that ED LOS was affected to a rate of 61.9% (p=0.029).
The greatest influence in ED LOS of polytrauma patient seemed to be the duration of x-rays and u/s studies (p= 0.028), the duration of CT studies (p=0.028) and the total time spent to complete diagnostic examinations in each case (p=0.026) (Table 2).
According to Spearmans’ Rho criterion it was estimated that polytrauma patients’ ED LOS was influenced directly by patients’: SpO2 (p=0.017), RTS (p=0.048), the duration of CT scan (p=0.002), the total duration of diagnostic examinations asked in each case (p=0.004), the number of medical specialists needed to evaluate each patient (p=0.001) and the waiting time for evaluation of all medical specialists (p=0.002) (Table 3).

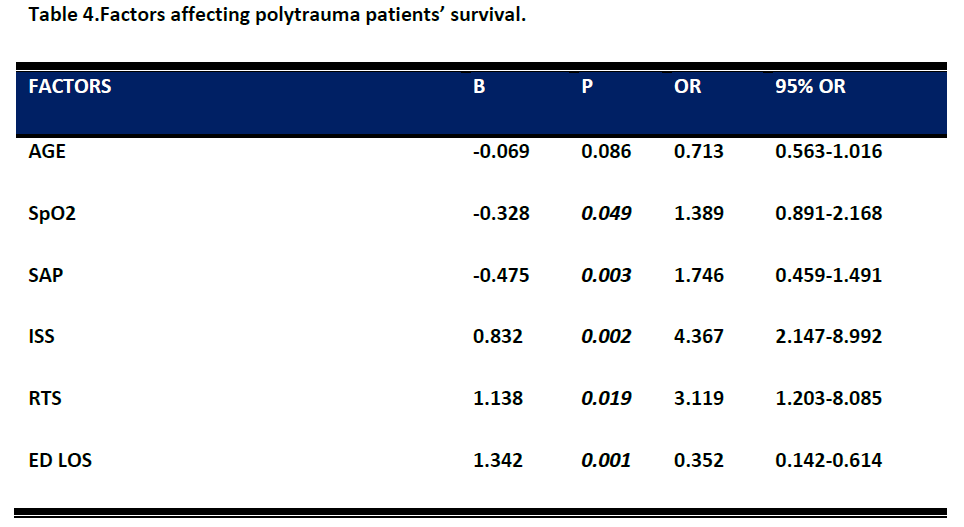
The factors examined for influencing patients’ outcome by applying multivariate logistic regression were the following: age, SpO2, SAP, ISS, RTS and ED LOS.
Factors found having statistically significant difference (p<0.05) and affect patients’ outcome were:
• ED LOS. Increased ED LOS decreased by 0.352 times patients’ chance of survival.
• SpO2. Patients with SpO2 less than 96% had 1,389 times greater chance of dying.
• SAP. Increased SAP by 10 mm Hg increased the chance of survival by 1,746 times.
• ISS. Increased ISS by 1 unit decreased the chance of survival by 4,367 times.
• RTS. Increased RTS by 1 unit decreased the chance of survival by 3,119 times (Table 4).
Discussion
The results of the present study showed that by modifying the number of medical specialists that were needed to evaluate patients and the waiting time to complete the evaluation, ED LOS was affected by 61.9% (p=0.029). Also, it was concluded that factors influencing polytrauma patients’ ED LOS were the number of x-rays and the time needed to complete them in each patient along with the abdominal u/s (p=0.028), the time needed for CT scan (p=0.028) and the total time for the diagnostic tests (p=0.026). Moreover, patients’ RTS (p=0.048) and SpO2 (p=0.017) were proved to affect directly their ED LOS. Last but not least, our study revealed that polytrauma patients’ survival was greatly influenced by SpO2 (p=0.049), SAP (p=0.003), ISS (p=0.002), RTS (p=0.019) and ED LOS (p=0.001).Moreover, we have come across some interesting results about the impact of specialty consulting on polytrauma patients’ treatment in the ED and on their ED LOS.
In a study conducted by Mowery et al., [17] it was estimated that for each medical specialist’s assessment of the patient, 30 min was added in the ED LOS. Though, in Austria and in Germany the polytrauma patient’s complete management was provided by a general surgeon – traumatologist. [18-21] In Switzerland and in the Netherlands, general surgeons not only receive and evaluate trauma patients but also undertake and deal with orthopaedic fractures. [18]
Another similar study that was undertaken by Margulies et al., [22] showed that provided care in the ED by a general surgeon – traumatologist that also deals with orthopaedic fractures, was advantageous in both time and money, without lacking in quality or safety. Similarly, according to Matsushima et al., [23] the presence of an emergency surgery specialist offered safe and rapid response to the admitted trauma patients. Moreover, in another research conducted by Handel et al., [24] it was proved that the presence of a coordinator who examined patients and realized diagnostic tests before surgeon’s examination in the ED reduced ED LOS 40 min.
As far as the diagnostic tests, the time needed to complete them and their impact on polytrauma patient’s ED LOS, Yoon et al., [25] estimated that ordering an u/s examination added 4.7 h to patient’s ED LOS, laboratory tests added 2.1 h, simple x-rays 1h and CT scan 0.7 h. Additionally, in the same study nursing or medical consulting also found to increase ED LOS.
Furthermore, in a study conducted Mowery et al., [17] it was revealed that ED LOS was affected by the time needed to complete an MRI in patients with vertebral fractures. ED LOS for these patients was between 6 to 16 hours. Also, specialty consulting was the strongest factor affecting patients’ ED LOS.
Another similar research that was undertaken by Davis et al., [26] concluded that performing a CT scan or other imaginary studies (i.e. angiography) and the time needed for trauma team to manage polytrauma patients in the ED increased ED LOS. On the other hand, the amount of simple x-rays and specialty consulting for each patient found to have a lower impact on ED LOS. Wurmb et al., [27-28]
conducted two studies in which they proved that checking polytrauma patient with CT whole body lasted 23 min while the use of conventional protocol, including abdominal u/s, chest x-ray and CT scan focused in selected anatomical regions of patient’s body consumed 82 min.
As far as factors affecting trauma patient’s survival are concerned, Mowery et al., [17] conducted a study in which they estimated that each additional hour in patients’ ED LOS increased hospital mortality. Also, the results of the same study showed that 8.3% of the sample who had ED LOS between 4 to 5 hours died. More specifically, for every 3 minutes that ED LOS was increased the possibility of dying increased by 1%.
Another similar research that was undertaken by Varma et al., [29] revealed that age over 20 years old, male sex, ISS>15, multiple injuries, brain injuries with neurological deficit and additional dysfunctions were related with early mortality in patients with vertebral column injuries.
Furthermore, Emircan et al., [30] concluded that: age, hypotension, abnormal breath rate, high ISS, low GCS and RTS, blunt trauma and additional abdominal injuries affected 307 patients’ with chest injury survival by 50%. In another study conducted by Eid et al., [31] on patients with brain injuries, it was found that ISS and hypotension reduced their chance of survival.
Similarly, Costa et al., [32] proved that as ISS increased in patients with ISS>15, mortality increased equally with statistically significant difference in relation with factors such as age, forces acted in injured region and total length of stay in hospital. Moreover, Carr et al., [33] estimated that each additional hour of patients’ ED LOS increased possibility of developing pneumonia by 20%.
However, ED LOS was related with mortality in the first 30 days of hospitalization for non trauma patients. [34-35] Thus, ED LOS of trauma or non trauma patients is very important and studies evaluating patients’ time-to-treatment in ED could be useful tools for improving provided care in this department. [36-38]
Conclusions
Polytrauma patients’ ED LOS, which is equal with their time-to-treatment, was proved to be influenced by the number of medical specialists needed to consult each patient along with the time needed to complete this procedure and also the duration of the diagnostic tests realized during patients’ management. For each unit of MAP increase of patients, ED LOS was increased 3,5 times. Polytrauma patients’ survival was related with SpO2, SAP, ISS, RTS and of course ED LOS.
3065
References
- Saluzzo F, Mayer A. Emergency department management, Theory of Continuous Quality Improvement. St.Louis, Missouri, Mosby, 1997.
- Walsh M & Kent A. Accident & Emergency Nursing 4th edition. Edinburgh, Butterworth-Heinemann, 2003.
- Παπαδαντωνάκη Α. Τμήμα Επειγόντων και Ατυχημάτων–Επιπτώσεις της Διαμόρφωσης του Χώρου στην Αντιμετώπιση των Ασθενών– Νοσηλευτική Προσέγγιση, Αθήνα: Εθνικό και Καποδιστριακό Πανεπιστήμιο Αθηνών, Τμήμα Νοσηλευτικής – Διδακτορική Διατριβή, 1989.
- Putsep E. Modern Hospital International Planning Practices. London, Lloyd-Luke, 1981.
- Ρούσσος Χ. Εντατική Θεραπεία Τόμος 3ος, 3η Έκδοση. Αθήνα, Πασχαλίδης, 2009.
- Greenspan L, McLellan B, Greig H. Abbreviated Injury Scale and Injury Severity Score: A Scoring Chart. J Trauma. 1985;25:60-64.
- Baker P, O'Neill B, Haddon W, Lon B. The Injury Severity Score: A Method for Describing Patients with Multiple Injuries and Evaluating Emergency Care. J Trauma. 1974;14:187-196.
- Tien H, Jung V, Pinto L, Mainprize T, Scales D, Rizoli S. Reducing time-to-treatment decreases mortality of trauma patients with acute subdural hematoma. Annals of Surgery. 2011;253:1178-1183.
- Jordan J. Coding for emergency department services. Ann Emerg Med. 1997;28:671-676.
- Committee on Trauma Task Force: Quality assurance in trauma care. In American College of Surgeons. Resources for Optimal Care of the Injured Patient. Chicago, 2006.
- Lerner E, Moscati R. The golden hour: scientific fact or medical ‘urban legend’?. Acad Emerg Med. 2001;8(7):758-60.
- Cowley R. Trauma Center. A new concept for the delivery of critical care. J Med Soc NJ. 1977;74(11):979-87.
- Lockey D. Prehospital trauma management. Resuscitation. 2001 Jan;48(1):5-15.
- Trunkey D. Trauma. Accidental and intentional injuries account for more years of life lost in the U.S. than cancer and heart disease. Among the prescribed remedies are the improved preventive efforts, speedier surgery and further research. Sci Am. 1983 ;249:28-35.
- Newgard C, Schimcker R, Hedges J, Trickett J, Davis D, Bulger E et al. Emergency Medical Services Intervals and Survival in Trauma: Assessment of the “Golden Hour” in a North American Prospective Cohort, Annals of Emergency Medicine. Ann Emerg Med. 2010;55(3):235-46.
- Marquis S. Da shock traumatique dans les blessures de Guerre-Analysis d’observations. Bull Med soc Chir. 1918 ;44:205.
- Mowery N, Dougherty S, Hildreth A, Holmes J, Chang M, Martin S et al. Emergency department length of stay is an independent predictor of hospital mortality in trauma activation patients. J Trauma. 2011;70(6):1317-25.
- Allgower M. Trauma systems in Europe. American Journal of Surgery. 1991;161(2):226-9.
- Kim J, Moore E, Moore F, Read R, Burch J. Trauma surgeons can render definitive surgical care for major thoracic injuries. J Trauma. 1994;36(8):871-5.
- Trunkey D. What’s wrong with trauma care? , Bulletin of the American College of Surgeons 1990;75:10-15.
- Haas N, Hoffman R, Mauch C, von Fournier C, Sudkamp N. The management of polytraumatized patients in Germany. Critical Orthopaedics and Related Research. 1995;318:25-35.
- Margulies D, Cohen M, Hiatt J. Emergency management of multisystem injuries by a surgical trauma surgeon. Injury. 1999;30(7):463-6.
- Matsushima K, Cook A, Tollack L, Shafi S, Frankel H. An acute surgery model provides safe and timely care for both trauma and emergency general surgery patients. Journal of Surgical Research. 2011;166(2):143-7.
- Handel A, O.John M, Workman J, Rongwei F. Impact of an expeditor on emergency department patient throughput. Western Journal of Emergency Medicine. 2011;12(2):198-203.
- Yoon P, Steiner I, Reinhardt G. Analysis of factors influencing length of stay in the emergency department. CJEM-JCMU. 2003;5(3):155-61.
- Davis B, Sullivan S, Levine A, Dallara J. Factors affecting ED length-of-stay in surgical critical care patients. American Journal of Emergency Medicine. 1995;13(5):495-500.
- Wurmb T, Fruehwald P, Hopmer W, Koewer N, Brederlan T. Whole-body multislice computed tomography as the primary and solid diagnostic tool in patient with blunt trauma searching for its appropriate indication .Am J Emerg Med. 2007;25(9):1057-62.
- Wurmb E, Frühwald P, Hopfner W, Keil T, Kredel M, Brederlau J et al. Whole-body multislice computed tomography as the first line diagnostic tool in patients with multiple injuries: the focus on time. J Trauma. 2009;66(3):658-65.
- Varma A, Hill E, Nicholas J, Selassie A. Predictors of early mortality after traumatic spinal cord injury. Spine. 2010;35(7):778-83.
- Emircan S, Ozguc H, Akkose Aydin S, Ozdemir F, Koksal O, Bulut M. Factors affecting mortality in patients with thorax trauma. Turkish Journal of Trauma & Emergency Surgery. 2011;17(4):329-33.
- Eid H, Barss P, Adam S, Torab F, Lunsjo K, Grivna M et al. Factors affectin anatomical region of injury, severity, and mortality for road trauma in a high-income developing country: Lessons for prevention. Injury. 2009;40(7):703-7.
- Costa G, Tomassini F, Tierno S, Venturini L, Frezza B, Cancrini G et al. The prognostic significance of thoracic and abdominal trauma in severe trauma patients (Injury Severity Score>15). Ann Ital Chir. 2010;81(3):171-6.
- Carr B, Kaye A, Wiebe D, Gracias V, Schwab C, Reilly P. Emergency department length of stay: a major risk for pneumonia in intubated blunt trauma patients. J Trauma. 2007;63(1):9-12.
- Chalfin D, Trzeciak S, Likourezos A, Baumann P, Dellinger R. DELAY-ED study group. Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit. Crit Care Med. 2007;35(6):1477-83.
- Parkhe M, Myles P, Leach D, Maclean A. Outcome of emergency department patients, with delayed admission to an intensive care unit. Emerg Med (fremantle). 2002;14(1):50-7.
- Ramsey F. Enhancing patient flow. In: Hellstern R. Managing the emergency department: a team approach. Dallas, American College of Emergency Physicians, 1992. 95-104p.
- Kyriacou D, Ricketts V, Dyne P, McCollough M, Talan D. A 5-year time study analysis of emergency department patient care efficiency. Ann Emerg Med. 1999;34(3):326-35.
- Rayner H. Length of stay. Taking a day off. Health Serv J. 1998 8;108(5585):32-3.

