Keywords
EMB; Expandable micro-motor bur; Molar tooth; Tooth root extraction
Introduction
Tooth extraction is a traumatic procedure often resulting in immediate destruction and loss of alveolar bone and surrounding soft tissues. A complex cascade of biochemical and histologic events then ensues during the wound healing process which further leads to physiologic alterations to the alveolar bone and soft-tissue architecture [1,2]. Expandable micro-motor bur (EMB) is a practical dental instrument proposed for the removal of broken teeth roots that cannot be extracted by the routine closed methods [3-6]. The device comprises a micro-motor, spacers, needles, bur base, and a round bur that drills halfway through the root canal, expands to make a spherical cavity around itself, and behaves as an efficient extraction aiding anchor. The utilization of EMB would introduce a new technique in the removal of broken teeth roots in which surgical trauma is minimized and so are post-extraction disorders [7-15]. The use of EMB would also eliminate surgical invasion to the surrounding tissues, and it would eliminate profound hand forces by the practitioner, consequently reduces stress for both the practitioner and the patient. It would also eliminate high-risk aftermaths of the surgery such as operative morbidity (due to bone loss), maxillary sinus exposure, and probable need for additional surgery which are some of the implications of the conventional open access approaches [16-20].
EMB tools
The structural components of EMB are: 1) Bur Head which consists of Split round bur and Hallow grooved shaft and 2) Bur base which consists of Spiral grooved shaft, Spacers, and Main shank. A micro motor would also power its spin. Figure 1 provides a demonstration of the EMB [21].
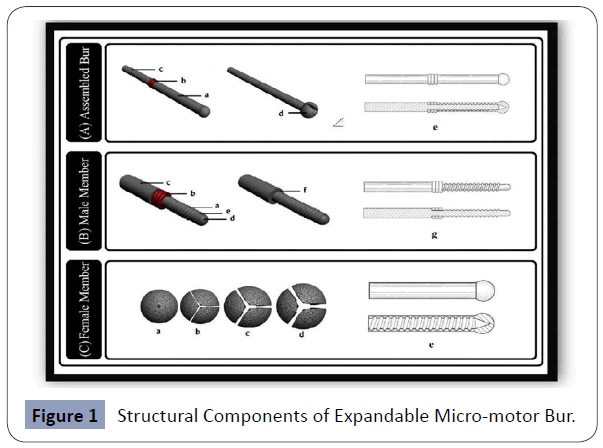
Figure 1 Structural Components of Expandable Micro-motor Bur.
In the Figure 1, picture (A) shows bur components in a position which are clutched together for mounting to micro-motor through the Main shank : (a) Bur head (female member), (b) Spacers, (c) Bur base (male member), (d) Expanded Bur Head, and (e) the cross-section view of the assembled bur. Picture (B) demonstrates the bur base (male member) and provides details about its components: (a) Spiral grooved shaft, (b) Spacers, (c) Main shank; (d) The round tip portion, (e) Male member without spacers, and (f) the cross-section view of the male member. Picture (C) shows the bur head (female member) and gives a top view of the round bur spinning in the root canal (a-d). Depending on the number of spacers, different degrees of expansion occur in the canal while spiral grooved shaft bears. These different degrees of expansion are shown when (a) three, (b) two, (c) one, (d) no spacers are on. (e) The cross-section view of the female member [18,19,21].
Materials and Methods
We have tested the prototype of EMB on the molar tooth root of 5 dogs in their upper jaw (M1) in the Medical Sciences and Technologies Research Institute of Shahid Beheshti University. and used as a baseline reference.
Supragingival scaling was performed on all dogs 5 days before tooth root extraction at each surgical session, the animals were pre-anesthetized with atropine 0.02 mg/kg i.v and anesthetized with 0.04 mg/kg medetomidine. And 5 mg/kg of ketamine-50 mixed in a syringe and administered i.m. 10 min after premedication and maintained with 2–3% Isoflurane-Vet and O2 at 95% and kept with an intravenous fluid of 0.9% saline solution 10 ml/kg/h. Local anesthesia was also provided. Blood pressure and O2 perfusion were constantly monitored.
EMB Operation
Details of the implementation of EMB to remove a broken tooth root are schematically presented stepwise in Figure 2. These operation steps are explained below:
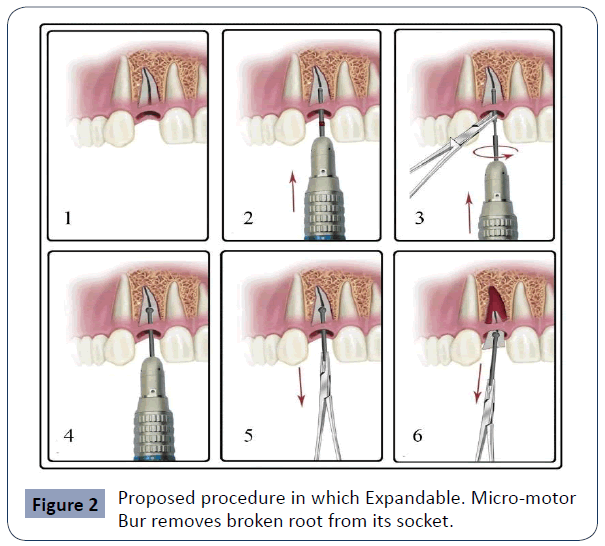
Figure 2 Proposed procedure in which Expandable. Micro-motor Bur removes broken root from its socket.
1. It shows a broken root that is already retained in its socket before the operation. 2.Using a micro-motor, a round bur will be drilled about halfway through the root canal, similar to a conventional bur while spacers are on. 3. Spinning stops; the micro-motor is detached from EMB; round bur is unscrewed from the bur base; spacers are reduced or totally removed (depending on the expansion degree required); round bur is placed back into the canal; bur base is mounted on micro-motor, by the help of a needle holder; round bur and bur base are screwed back. Round bur carves its periphery making a spherical cavity around itself. This step is run for a very short period. 4. Spinning stops; micro-motor is detached and EMB remains in place. While expanded in the root canal, the split round bur behaves as an efficient extraction-aiding anchor. 5,6. The firm anchor eases the extraction of the broken root with the help of a needle holder [21].
Results
Radiographic images after the molar tooth root surgery are shown in Figure 3 and Figure 4. No injuries to the buccal bone and surrounding nerves were observed and the root was successfully extracted. Figure 5 shows the damages to the jaw and teeth root surroundings of another dog in open surgery [22].
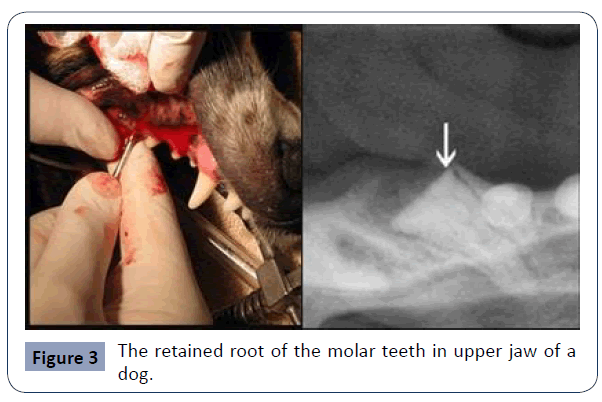
Figure 3 The retained root of the molar teeth in upper jaw of a dog.
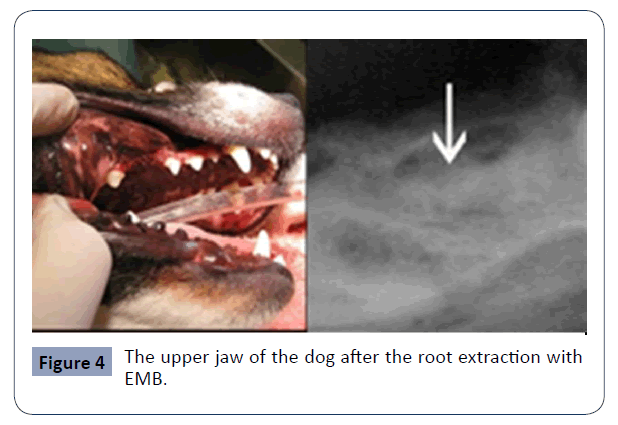
Figure 4 The upper jaw of the dog after the root extraction with EMB.
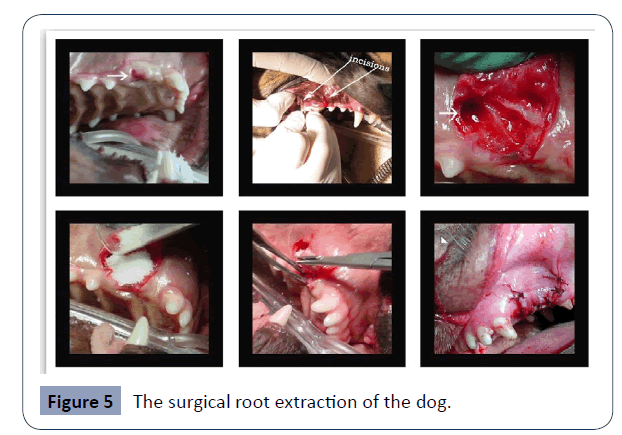
Figure 5 The surgical root extraction of the dog.
The results show that invasion to surrounding anatomical structures (maxillary sinus exposure, nerve injury, and innervation disorders) in the EMB method is less probable compared to the Conventional Technique and similarly need for the mucoperiosteal flap and/or osteotomy of buccal bone in using EMB is None or with less extension. The Surgical approach of Conventional Techniques More invasive while the EMB approach seems more conservative. Operation duration in the Conventional Technique is more than the EMB method. The other result that can derive from the test is that the risk of exposing high pressure to adjacent teeth in the EMB method is less than other Conventional Techniques, and less healing time is observed due to use of EMB bur in comparison with conventional methods.
Conclusion
Considering the application of this treatment, further studies are needed to confirm its effect in more clinical cases. The likelihood of its negative influence on nearby vascular and nerve system should be well evaluated. When these concerns are clear, we believe that EMB could be used as a new tool to assist removal of broken teeth roots in humans.
36388
References
- Almer MH (1969) The time sequence of tissue regeneration in human extraction wounds. Oral Surg Oral Med Oral Pathol 27:309-318.
- Cardaropoli G, Araujo M, Lindhe J (2003) Dynamics of bone tissue formation in tooth extraction sites: an experimental study in dogs. J Clin Periodontol 30:809-819.
- Nageshwar RD (2002) Common incision for impacted mandibular third molars. J Oral Maxillofac Surg 60: 1506-1509.
- Quee TA, Gosselin D, Millar EP, Stamm JW (1985) Surgical removal of the fully impacted mandibular third molar. The influence of flap design and alveolar bone height on the periodontal status of the second molar. J Periodontol 10: 625–631.
- Sutherland KJG (1963) Mucoperiosteal flaps in dento-alveolar surgery. Aust Dent J 6: 317-325.
- Capuzzi P, Montebugnoli L, Vaccaro MA (1994) Extraction of impacted third molars. A longitudinal prospective study on factors that affect postoperative recovery. Oral Surg Oral Med Oral Pathol 77: 314-323.
- Garcia AG, Sampedro FG, Rey JG, Torreria MG (1997) Trismus and pain after removal of impacted lower third molars. J Oral Maxillofac Surg 55: 1223-1226.
- Stephen RJ, App GR, Foreman DW (1983) Periodontal evaluation of two mucoperiosteal flaps used in removing impacted mandibular third molars. J Oral Maxillofac Surg 41: 719-725.
- Groves BJ, Moore JR (1970) The periodontal implications of flap design in lower third molar extractions. Dent Pract Dent Rec 20: 297-304.
- Rosa AL, Carneiro MG, Lavrador MA, Novaes AB (2002) Influence of flap design on periodontal healing of second molars after extraction of impacted mandibular third molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 93: 404-409.
- Suarez-Cunqueiro MM, Gutwald R, Reichman J, Otero-Cepeda XL, Schmelzeisen R (2010) Marginal flap versus paramarginal flap in impacted third molar surgery: A prospective study. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 95: 403–408.
- Dostalova T, Seydlova M (2010) Dentistry and Oral Diseases for Medical Students. HavlickuvBrod, Czech Republic: Grada Publishing.
- Van der Weijden F, Dell Acqua F, Slot DE () Alveolar bone dimensional changes of post-extraction sockets in humans: a systematic review. J Clin Periodontol36:1048-1058.
- Jakse N, Bankaoglu V, Wimmer G, Eskici A, Petl C (2002) Primary wound healing after lower third molar surgery: Evaluation of two different flap designs. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 93: 7-14.
- Clauser C, Barone R (1994) Effect of incision and flap reflection on postoperative pain after the removal of partially impacted mandibular third molars. Quintessence Int 25: 845-849.
- Garcia AG, Sampedro FG, Torrella MG, Vila PG, Madrinan-Grana P, et al. (2001) Trismus and pain after removal of a lower third molar. Effects of raising a mucoperiosteal flap. Med Oral 6: 391-396.
- Penarrocha M, Sanchis JM, Saez U, Gay C, Bagan VJ (2001) Oral hygiene and postoperative pain after mandibular third molar surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 92: 260-264.
- Retzepi M, Donos N (2010) Guided Bone Regeneration: biological principle and therapeutic applications. Clin Oral Implants Res 21: 567-572.
- Stephens JR, App GR, Foreman DW (1983) Periodontal evaluation of two mucoperiosteal flaps used in removing impacted mandibular third molars. J Oral Maxillofac Surg 41: 719-725.
- Charles AK, Ramfjord SP (1960) Healing of gingival mucoperiosteal flaps. Oral Surg Oral Med Oral Pathol 13: 89-103.
- Wadhwani KK, Garg A (2004) Healing of soft tissue after different types of flap designs used in periapical surgery. Endodontology 16: 20-22.
- Bonjar AHS (2013) Expandable Micro-motor Bur, design of a new device for least invasive extraction of broken teeth roots. Annals of Surgical Innovation and Research 7:1-5.

