Keywords
Peer-led, health education, cigarette smoking, adolescents
Introduction
A wide range of tobacco products enjoy global use, the most frequently consumed form being cigarettes [1]. Cigarette may be the only legally available consumer product that is harmful to one’s health when used as intended by the manufacturers. Cigarette smoking has been described as the world’s fastest spreading and longest lasting epidemic [1].
Cigarette smoking usually commences during adolescence and continues into adult life, meaning that many tobacco’s future victims are today’s children [2,3] adolescent cigarette smoking increases the risk for long term regular adult smoking, [3,4] individuals who do not initiate cigarette smoking before the age of 20 years are not likely to become adult smokers [5].
Cigarette smoking is one of the major preventable causes of death in the world today.
Cigarette smoking kills about a third to a half of all smokers [6]. Annually an estimated 4 million cigarette smokers die worldwide [7] half of these deaths are already occurring in developing countries [8]. Epidemic of cigarette smoking is already shifting from the developed countries to the developing countries [3,4,9,10] by the year 2030, 70% of deaths due to cigarette smoking worldwide would come from developing countries [7]. This may be as a result of aggressive marketing by cigarette manufacturers in Nigeria and other developing countries coupled with lack of implementation of tobacco control policies. If no action is taken, Nigeria, with a 2013 projected population of 144 million people could face a grim future regarding tobacco related disease and death [11,12].
A young person’s peer has great influence on the way he or she behaves. This is true of both risky and safe behaviour. Peer education makes use of peer influence in a positive way. Several studies have shown that peer education can improve adolescents knowledge, provide positive attitude and behaviour [13,14]. It is against this background that this study instituted a peer led health educational intervention in an attempt to improve cigarette smoking related knowledge, provide positive smoking related attitude and behaviour among in-school adolescents in Sokoto metropolis, Nigeria.
It is hoped that this intervention will reduce cigarette smoking initiation in adolescents, and in turn play a great role in reducing the morbidity, mortality, disability and economic burden associated with cigarette smoking. It is also hoped that the students selected for the educational intervention will conduct peer led step down trainings for their colleagues in their respective schools which will further improve the adolescent students cigarette related knowledge, attitude and behaviour.
Methodology
This study was conducted between February and July 2012 in 4 metropolitan Local Government Areas (LGAs) of Sokoto state, North West, Nigeria. These LGAs were Sokoto North, Sokoto South, Wammako and Dange-Shuni LGAs. The study recruited 20 senior secondary schools in Sokoto metropolis; owned by the Federal Government (2), Sokoto State Government (12) and the rest by private individuals (6). There were 15,702 students in these senior secondary schools.
The study was a quasi- experimental design comparing the study and control groups (with pre and post intervention data collection). This study design made use of a study and control (comparison) group so that any difference observed post intervention within the study group, as well as between the two groups, post intervention can be attributed to the health education intervention given.
The study population comprised all adolescents (10-19 years) studying in senior secondary schools in Sokoto metropolis. All the schools were stratified into 3 strata (Federal, State and Private schools). Proportional allocation based on the number of schools in each stratum was done. Using the formula to compare proportions in 2 independent groups (study and control) with pre and post test [15] and a prevalence of 53.8% from a previous study, [16] a total of 114 students were recruited for each of the study and control groups using two stage sampling technique.
Data was collected by administering a 44 itemed self-administered questionnaire modified from the core questions of the Global Youth Tobacco Survey (GYTS). The instrument contained 4 sections which sought information on respondents’ demographic characteristics (e.g. age, sex, ethnicity etc.), cigarette smoking related knowledge (e.g. knowledge of the different disease conditions cigarette smoking is associated with), attitude (e.g. attitude towards allowing smokers to smoke in public etc.) and behaviour (e.g. respondents buying and smoking of cigarette within 30 days prior to the survey). The questionnaire was administered to the respondents before and after the peer led health education intervention by trained research assistants. Pairing of individual respondent’s questionnaire was done pre and post-intervention so that each individual respondent’s pre-intervention score can be compared with the post- intervention scores.
The data collection and intervention were conducted in all the schools on separate days. The intervention consisted of 2 peer led health education sessions administered to respondents in the study group only. Each session consisted of a didactic lecture (which sought to improve respondents’ knowledge, provide positive attitude and behaviour with regard to cigarette smoking) and showing an 18 minute video clip, which dramatized the harmful effects of cigarette smoking. After the video clip, there was an interactive discussion with the respondents during which questions were entertained and answered. Each session lasted about 60 minutes and was repeated 4 weeks after the first health education intervention. The study participants were also exposed to posters and hand bills to reinforce the health education message. Post intervention data collection was obtained 3 months after the second health education intervention.
The questionnaires were entered into and analyzed using SPSS statistical software package version 17. Respondents’ cigarette smoking related knowledge were graded and scored, each correct response was given one score and any wrong or non response was not given any score. Paired t test was used to determine the relationship between the pre and post-interventions mean knowledge score of the respondents. McNemar Chi square test was used to determine the statistical significance of the difference in the pre and post intervention stage of the study. Results were presented in form of tables. All statistical tests were carried out using 2 tailed tests with alpha set at 0.05.
Approval for this study was sought and obtained from the ethical committee of Usmanu Danfodiyo University Teaching Hospital (UDUTH) Sokoto. Permission to carry out the study was obtained from heads of respective schools and informed consent was obtained from the students and guardians/parents.
Results
In the study group, all of the 114 (100%) respondents recruited for the study attended the first health education intervention. However of the 114 respondents who attended the first intervention, 111 (97.4%) respondents attended the repeat health education intervention. Post intervention data was obtained from 109 (95.6%) respondents in the study group who attended both health education interventions (respondents in the study group who did not attend both interventions were not given questionnaires to fill), and 112 (98.2%) respondents in the control group who turned up for the survey.
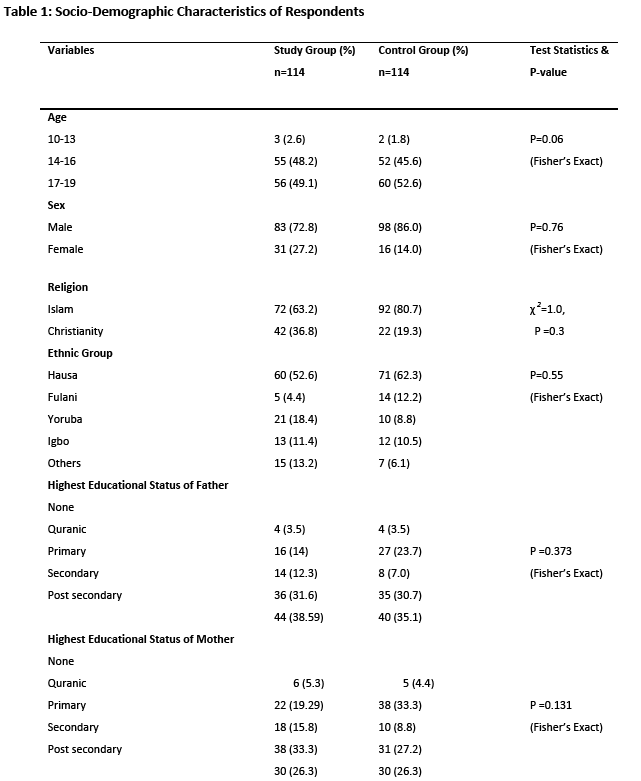
Respondents in both the study and control group were comparable with respect to their socio demographic characteristics. Forty nine and fifty three percent of the respondents in the study and control groups were of the age group 17-19 years. The mean age of the respondents in the study and control groups was 16±1.6 years and 17±1.7 years respectively. Majority of the respondents, (study 72.8% and control 86%) were males and Muslims (study 63.2% and control 80.7%). About half of the respondents in the study group 60 (52.6%) and most of the respondents in the control group 71 (62.3%) were Hausas (P=0.55).
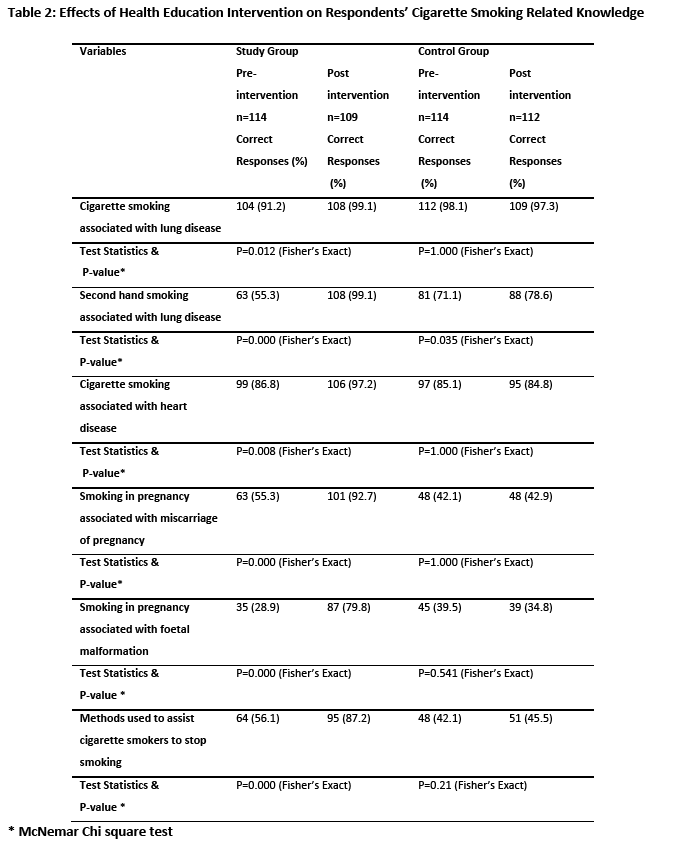
Majority of respondents (91.2%) in the study group at baseline knew that cigarette smoking is associated with lung disease, this proportion increased to 99.1% after intervention (P=0.012). At baseline, in the study group, 55.3% of respondents could associate second hand cigarette smoking with lung disease, this proportion increased to 99.1% after intervention (P=0.000). Less than a third of respondents in the study group 35 (28.9%) could correctly associate cigarette smoking in pregnancy with foetal malformation before intervention, this proportion increased to 79.8% after intervention (P=0.000). Slightly more than half (56.1%) of respondents in the study group at baseline knew the correct means of assisting cigarette smokers to stop smoking this increased to 87.2% at post-intervention.
In the study group, the mean knowledge score of respondents increased from 61.24 before the intervention to 92.31 after the intervention, this increase was found to be statistically significant (P=0.000).
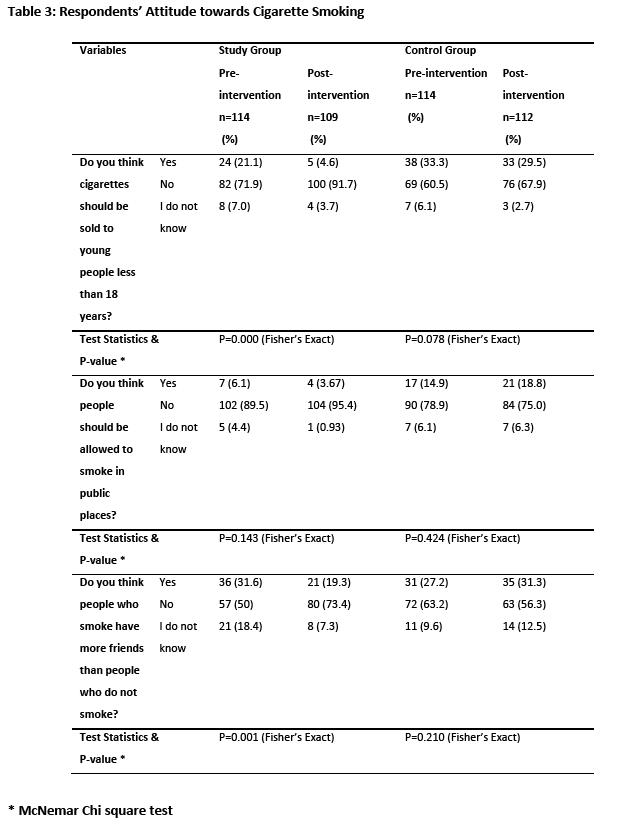
More than two thirds (71.9%) of respondents in the study group at baseline did not feel that cigarettes should be sold to people less than 18 years old, this increased to 91.7% post-intervention (P=0.000). More than three quarters (89.5%) of respondents in the study group at baseline did not feel that people should be allowed to smoke in public places, this proportion increased to 95.4% post-intervention (P=0.143).
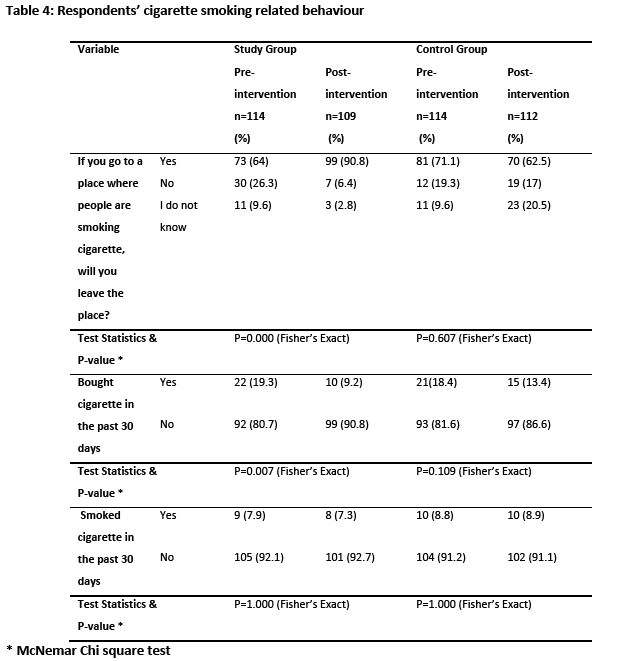
Pre-intervention 64% of respondents in the study group reported that they would leave a place where cigarette is being smoked, this proportion increased to 91% post-intervention (P=0.000). In the study group, 19.3% of respondents had bought cigarette in the month before the baseline survey, this proportion decreased in the study group to 9.2% post intervention (P=0.007). Pre-intervention, 7.9% of respondents had smoked in the month preceding the data collection, this proportion decreased to 7.3% at post intervention (P=1.000).
Discussion
Most of the respondents in the study and control groups were in the age range of 17-19 years. This is because of the 6-3-3-4 educational structure of Nigeria where children start primary school by the age of 6 years; spend 6 years in primary school, 3 years each in junior and senior secondary school and 4 years in the university.
At base line a high proportion of respondents in both the study group and control group knew that cigarette smoking is associated with lung disease (Table 1). This is much higher than figures obtained from previous studies conducted in various parts of Nigeria. Studies conducted in north central [17] and south west [18] Nigeria revealed that most of respondents in the study and control group could associate cigarette smoking with lung disease. Another study conducted North east Nigeria [16] reported that a third of respondents could associate cigarette smoking with lung disease respectively. Majority of our respondents in the study and control groups also had good knowledge on the association between cigarette smoking and heart disease. This result contrast with that of previous studies conducted in north central Nigeria where less than a quarter of the respondents in study and control groups respectively could associate cigarette smoking with increased blood pressure [17]. Other studies conducted in south west [19] and north east [16] Nigeria reported that less than half of the respondents respectively could associate cigarette smoking with heart disease.
In the study group, at baseline, majority of respondents did not feel that cigarettes should be sold to people less than 18 years old (Table 3), this contrasts with another study carried out in north central Nigeria where half of respondents felt cigarette should not be sold to young people [17]. Pre-intervention, in the study group, most of the respondents did not feel that people should be allowed to smoke in public places (Table 3). This finding is much higher than that reported by another study conducted in north east Nigeria where about half of respondents wanted smoking in public places banned [16].
At baseline more than half of the respondents in the study group reported that they would leave a place where cigarette is being smoked (Table 4). This figure is encouraging especially against the background of the harmful effect of environmental tobacco smoke. Our study also discovered that less than one-fifth of respondents in the study group had bought cigarette in the month before the baseline survey (Table 4). Pressure should be put on government to ban sale of cigarette to minors because adolescents who have access to cigarette are likely to also experiment with it, which may lead to regular smoking in adult life.
After the peer-led health education intervention given to the respondents in the study group, there was statistically significant increase in the proportion of respondents who could correctly associate cigarette smoking with lung disease; heart disease; miscarriage of pregnancy and fetal malformation, also there was a significant increase in the proportion of respondents who could correctly associate second-hand cigarette smoking with lung disease (Table 2). This significant increase can be attributed to the peer led health education intervention that was given to respondents in the study group as there was no corresponding increase among respondents in the control group. Several studies have also documented respondents increase in cigarette smoking related knowledge following intervention [17,20-22].
In the study group, after the intervention there was a significant increase in the proportion of respondents who felt cigarette should not be sold to young people; proportion of respondents who felt that people who smoke cigarette do not have more friends than those who do not smoke cigarette (Table 3). The significant improvement in the cigarette smoking related attitude of respondents in the study group may be attributed to the 2 sessions of health education intervention given them as well as the improvement in their cigarette smoking related knowledge. A previous study conducted in Nigeria reported that health education intervention was successful in improving cigarette smoking related attitude of respondents, [17] in contrast to another study carried out in Saudi Arabia where health education intervention was unable to improve respondents’ cigarette smoking related attitude [22].
It is encouraging to note that in the study group, there were fewer respondents who bought cigarette at post- intervention compared with those who bought cigarette at baseline (Table 4). Buying cigarettes, whether for themselves or for others provides these adolescents with opportunity to experiment with cigarettes and this act may lead to regular smoking later in life. At post intervention there were fewer respondents in the study group who reported smoking. We did not conduct cotinine assay of respondents, so we were not able to ascertain that respondents who did not report smoking had really stopped smoking. The peer led health education intervention was unable to get respondents who were already smoking cigarette to stop smoking. Some Peer led intervention programs have been found to be successful in improving adolescents cigarette smoking behaviour [13,14]. Smoking cessation programs have poor outcome, it is estimated that among smokers who try to quit only 2-3% succeed in stopping smoking permanently [23]. Peer led health education intervention was found to be successful in improving cigarette smoking related knowledge, attitude of respondents. It was also found to be successful in changing some of negative behaviour of respondents.
Conclusion
The peer-led health education intervention was found to be effective at improving cigarette smoking related knowledge, attitude and behaviour of the respondents. A sustained health education program should be established to improve in-school adolescents’ cigarette smoking knowledge, attitude and behaviour.
2626
References
- Can G, Topbas M, Oztuna F, Ozgun S, Can E. Factors contributing to regular smoking in adolescents in Turkey. Journal of School Health 2009; 79(3):93-7.
- Mpabulungi L, Muula AS. Tobacco use among high school students in Kampala,Uganda: Questionnaire study. Croatian Medical Journal 2004;45(1):80-3.
- Siziya S, Rudatsikira E, Muula AS. Cigarette smoking among school-going adolescents in Kafue, Zambia. Malawi Medical Journal 2007;19(2):75-8.
- Reddy KS, Perry CL, Stigler MH, Arora M. Differences in tobacco use among young people in urban India by sex, socioeconomic status, age, and school grade: Assessment of baseline survey data. Lancet 2006;367(9510):589-94.
- Chalela P, Velez LF, Ramirez AG. Social influences, attitudes and beliefs associated with smoking among border Latino youth. Journal of School Health 2007;77(4):187-95.
- World Health Organisation. World Health Statistics 2008. Geneva: 2008. Available online at www.who.int/whosis/whostat/2008/en/ [ Accessed 2011 13/3].
- Warren CW. Tobacco use among youth: A cross country comparison. Journal of Tobacco Control 2002;11(3):252-70.
- Owusu-Dabo E, Lewis S, McNeill A, Anderson S, Gilmore A. Smoking in Ghana: A review of tobacco industry activity. Journal of Tobacco Control 2009;18(3):206-11.
- Stebbins KR. Tobacco, politics and economics: Implications for global health. Journal of Social Science Medicine 1991;33(12):1317-26.
- Townsend L, Flisher AJ, Gilreath T, King G. A systematic literature review of tobacco use among adults 15 years and older in sub-Saharan Africa. Journal of Drug and Alcohol Dependence 2006;84(1):14-27.
- National Population Commission, Macro International. Nigeria demographic and health surveys 2008. Available online at https://www.unicef.org/nigeria/ng_publications_Nigeria_DHS_2008_Final_Report.pdf [Accessed 2011 13/3].
- National Population Commission. Projected figures of population and housing census of the Federal Republic of Nigeria: Population and housing tables 2006 Available from: www.population.gov.ng/[Accessed 2011 13/3].
- Campbell R, Starkey F, Holliday J, Audrey S. An informal school-based peer-led intervention for smoking prevention in adolescence: A cluster randomised trial. Lancet 2008;371(9624):1595-602.
- Lotrean L, Dijk F, Mesters I, Ionut C. Evaluation of a peer-led smoking prevention programme for Romanian adolescents. Journal of Health Education Research 2010;25(5):803-14.
- Jekel J, Katz D, Elmore J. Epidemiology, biostatistics and preventive medicine. 2 ed. Philadelphia, Pennsylvania: Saunders; 2001.
- Salawu FK, Danburam A, Desalu OO, Olokoba AB, Agbo J, Midala JK. Cigarette smoking habits among adolescents in Northeast Nigeria. Mera: African Journal of Respiratory Medicine 2009;8(1):8-11.
- Salaudeen AG, Akande TM, Musa OI. Effects of health education on cigarette smoking habits of young adults in tertiary institutions in a northern Nigerian state. Health Science Journal 2011;5(3):216-26.
- Adewole O, Folorun S, Obasoki D, Adosina, Erhabor G. Prevalence of smoking among secondary school students in Ile-Ife, Nigeria. Journal of Lung Cancer 2005;49(1):189-92.
- Osungbade KO, Oshiname FO. Determinants of cigarette smoking among senior secondary school students in a rural community of Southwest, Nigeria. Nigerian Journal of Medicine 2008;17(1):40-4.
- Hunter S, Steyn K, Yach D. Smoking prevention in black schools. A feasibility study. South African Journal of Education 1991;1(1):137-42.
- Lee FH, Wang HH. Effect of health education on prevention of smoking among eight-grade students. Kaosing Journal of Medical Science 2002;18(6):295-304.
- Abolfotouh MA, Aziz MA, Badawi IA, Alakija W. Smoking intervention programme for male secondary-school students in south-western Saudi Arabia Eastern Mediterranean Health Journal 1997;3(1):90-100.
- Aveyard P, West R. Managing smoking cessation. BMJ 2007;335(7609):37-41.

