Jeevan Naik, Krishnendu Choudhury* and Joydeep Das
Department of Pediatric Medicine, Jagannath Gupta Institute of Medical Sciences, Kolkata, West Bengal, India
- *Corresponding Author:
- Krishnendu Choudhury
Department of Pediatric Medicine
Jagannath Gupta Institute of Medical Sciences
Kolkata, West Bengal, India
Tel: +8145606690
E-mail: dkushal.ch2009@gmail.com
Received Date: August 16, 2021; Accepted Date: October 22, 2021; Published Date: October 29, 2021
Citation: Naik J, Choudhury K, Das J (2021) Vertebral Tumour Presenting with Progressive Flaccid Paraparesis and Areflexia in an Adolescent Girl. J Neurol Neurosci Vol.12 No.10:396
Ewing's Sarcoma (ES) is a rare malignancy but 2nd most common malignant tumor of long bones after osteosarcoma usually occurring in children and young adults. Rarely, it can affect vertebra or spine in adolescent masquarading as a progressive infectious lesion. The spinal ES usually occurs in lumbar vertebrae and presents with progressive neurological deficits in lower limbs. Ewing’s Sarcoma has poor prognosis because of uncontrolled metastatic potential making early diagnosis and intervention critical for survival of the patient. We report here a case of ES in a 14-year-old girl with involvement of lumbar spine with local spread and invasion of cauda equina with radiological, histopathological and immunohistochemical features.
Keywords
Ewing’s Sarcoma; Paraparesis; Tuberculous spineround cell tumor; Immunohistochemistry
Introduction
Ewing's sarcoma is a rare malignant round cell tumor that was first described by Ewing. It can occur in any bone but commonly it is found in the diaphysis of long bones and pelvic girdle [1]. It accounts for 4-10% of all primary bone cancers affecting adolescents and young adults. ES can rarely arise from the spine itself, usually in a vertebra, and present with progressive neurological deficits [2,3]. Early diagnosis is imperative to initiate appropriate treatment protocol.
Case Report
A 14 year old female presented with low back pain and paresthesia of both lower limbs for the last 7 months. There was no bladder or bowel disturbance. Because of paresthesia she had a fall 6 month back and had an L2 vertebral compression fracture; imaging at that time reveals a paravertebral mass (Figure 1) with infiltration of spinal thecal sac and exiting nerve roots below conus medullaris and nerve roots of cauda equina. The initial MRI report suggested tuberculous spine for which ATD (antituberculous drug) therapy was started as due to containment for coronavirus outbreak parents could not complete the biopsy and continued with ATD. There was no improvement after taking ATD for last 4 months. At present she developed severe low back pain and progressive weakness and numbness of both lower limbs when she was s brought to this hospital. On examination, there was anemia, edema both legs, her vital parameters including pulse, blood pressure, temperature and respiration were within normal range. Neurologically, power of both lower limbs was grade 0/5, with severe hypotonia and absent deep tendon reflexes. Plantar responses were mute bilaterally. Touch, pain, temperature, vibration and position sensations were absent in both lower limbs.
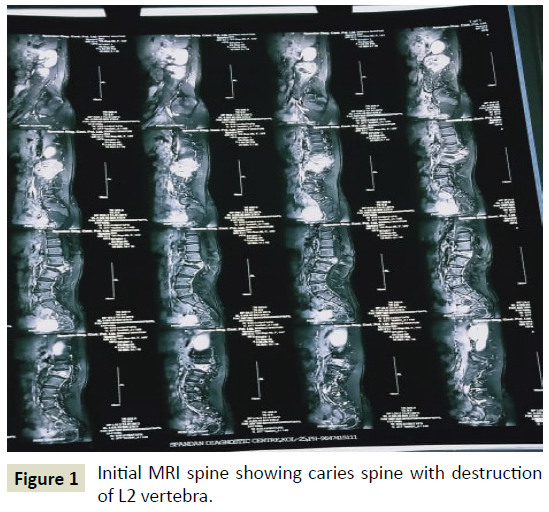
Figure 1: Initial MRI spine showing caries spine with destruction of L2 vertebra.
Radiological features (Figure 2) after admission suggested a destructive lesion in L-2 vertebral body with a suspicion of malignancy. Routine hemogram and biochemical examination revealed no abnormality. USG guided biopsy was done from the L-2 vertebral lesion after obtaining consent. Microscopy (Figure 3) revealed nests of round to oval cells having hyperchromatic nuclei and scanty cytoplasm surrounded by broad bands of fibrous tissue with foci of necrosis. Immunohistochemistry showed positivity to Mic-2, NKX-2.2, synaptophysin and immunonegative to cytokeratin, desmin, LCA,TdT which suggestive of malignant round cell tumor- Ewing's Sarcoma.
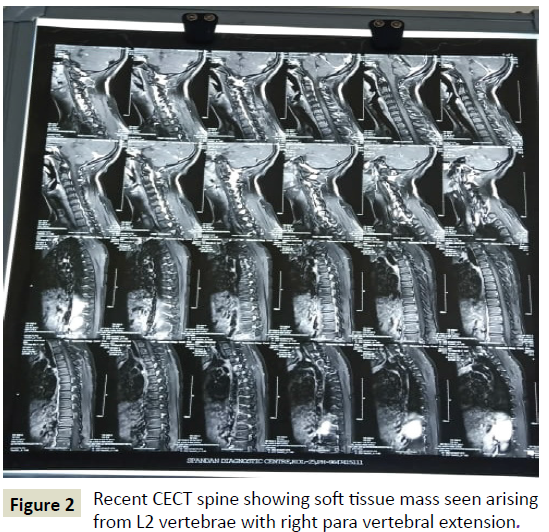
Figure 2: Recent CECT spine showing soft tissue mass seen arising from L2 vertebrae with right para vertebral extension.
Figure 3: Biopsy slide with histopathology and immunohistochemistry (confirmed Ewing sarcoma).
Discussion
In our patient the initial interpretation of the MRI scan by the radiologist was that of a destructive lesion in the vertebral body of the L2 vertebra most likely to be due to an infective process like tuberculosis [4]. As biopsy could not be done due to containment for coronavirus outbreak, the final diagnosis was delayed. Subsequently when the patient attended our hospital, USG guided biopsy was done and the report confirmed the lesion to be Ewing sarcoma.
Conclusion
Any child presenting with progressive weakness of both lower limbs should be evaluated for dorso lumbar spinal pathology including malignant tumor of vertebra. Early diagnosis with biopsy and immunohistochemistry is essential in ES to improve survival by treatment with surgery, radiotherapy and chemotherapy in combination.
41444
References
- Gopalokrishnan CV, Shrivastava A, Easwar HV, Nair S (2012) Primary Ewing's sarcoma of the spine presenting as acute paraplegia, J Pediatr Neurosci 7: 64–66.
- Goktepe A, Alaca R, Mohur H (2002) Paraplegia: An unusual presentation of Ewing's sarcoma. Spinal Cord 40: 367–369.
- Pilepich MV, Vietti TJ, Nesbit ME, Tefft M, Kissane J, et al. (1981) Ewing's sarcoma of the vertebral column. Int J Radiat Oncol Biol Phys 7: 27–31.
- Gijtenbeek JM, Van Den Bent MJ, Vecht CJ (1999) Cyclosporine neurotoxicity: A review. J Neuro 246: 339–346.

