Knapsis A, Schelzig H and Oberhuber A*
Department of Vascular and Endovascular Surgery, University of Duesseldorf, Germany
*Corresponding Author:
Alexander Oberhuber
Department of Vascular and Endovascular Surgery
University of Duesseldorf, Moorenstraße 5
40225 Duesseldorf, Germany.
Tel: 0211/81-19679
Fax: 0211/81-19091
E-mail: Alexander.Oberhuber@med.uniduesseldorf.de
Received Date: October 14, 2016; Accepted Date: October 17, 2016; Published Date: October 19, 2016
Citation: Knapsis A, Schelzig H, Oberhuber A. Visualization of an Aortic Coarctation, Induced by a Thoracic Stent Graft, Using 4D Magnetic Resonance Imaging. Ann Clin Lab Res. 2016, 4:4 doi: 10.21767/2386-5180.1000126
In 2001 a 13-year-old girl was taken to hospital after car accident, injured by multiple traumas, including an aortic rupture loco typico. Bleeding was brought under control via an endovascular approach with a Gore (W. L. Gore and Associates, Flagstaff, Ariz, USA) iliac limb 14-16-7. Follow-up CT scans showed over the years a relevant, but constant, bird-beak configuration of the stent graft. In 2009 the patient developed progressive arterial hypertension with a secondary hyperparathyroidism. For further investigation a conventional angiography with pressure gradient measurement and a four-dimensional magnetic resonance imaging was performed. The quantitative flow measurements were obtained by means of a retrospective ECG gated cardiacphase resolved three-dimensional T1 weighted fast gradient echo acquisition
Case Blog
In 2001 a 13-year-old girl was taken to hospital after car accident, injured by multiple traumas, including an aortic rupture loco typico. Bleeding was brought under control via an endovascular approach with a Gore (W. L. Gore and Associates, Flagstaff, Ariz, USA) iliac limb 14-16-7. Follow-up CT scans showed over the years a relevant, but constant, bird-beak configuration of the stent graft (Figure 1). In 2009 the patient developed progressive arterial hypertension with a secondary hyperparathyroidism. For further investigation a conventional angiography with pressure gradient measurement and a four-dimensional magnetic resonance imaging was performed. The quantitative flow measurements were obtained by means of a retrospective ECG gated cardiacphase resolved three-dimensional T1 weighted fast gradient echo acquisition [1,2].
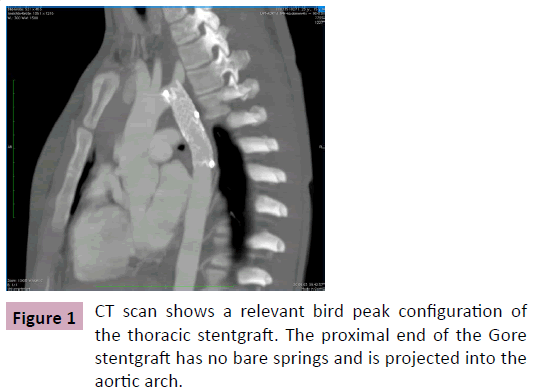
Figure 1: CT scan shows a relevant bird peak configuration of the thoracic stentgraft. The proximal end of the Gore stentgraft has no bare springs and is projected into the aortic arch.
The pressure gradient across the stent graft was 39 mmHg. Angiography showed a significant movement of the proximal end of the stent graft (Figure 2). The MRI confirmed the suspicion of a high-grade stenosis resulting in a functional coarctation. Flow analysis showed acceleration from 58 cm/s in the ascending aorta to 180 cm/s at the proximal end of the stent graft (Figure 3 and Video 1). The patient underwent open conversion with explantation of the stent graft and prosthetic graft insertion.
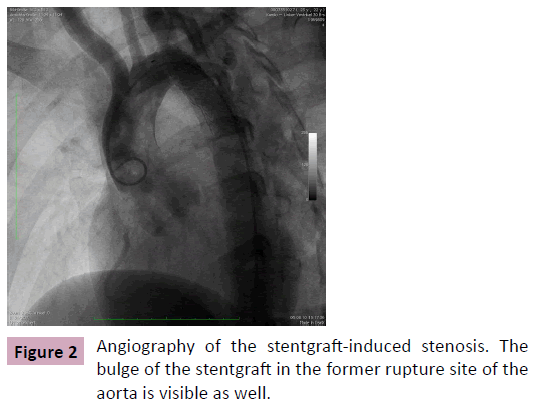
Figure 2: Angiography of the stentgraft-induced stenosis. The bulge of the stentgraft in the former rupture site of the aorta is visible as well.
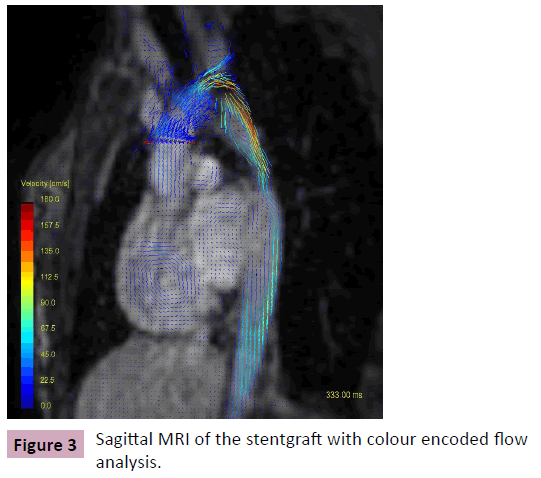
Figure 3: Sagittal MRI of the stentgraft with colour encoded flow analysis.

Video 1: HPLC chromatogram of the nine reference compounds in 50% aqueous methanol, measured at 370nm. Retention times for rutin, sutherlandin A, sutherlandin B, kaempferol-3-O-rutinoside, sutherlandin C, sutherlandin D, quercitrin, quercetin and kaempferol were 11.9, 12.7, 13.8, 15.3, 16.2, 17.0, 18.0, 26.2 and 28.1 minutes, respectively.
Funding
This work was supported by a grant from Gore (W. L. Gore and Associates, Flagstaff, Ariz, USA) and Medtronic (Medtronic World Medical, Sunrise, Fl, USA).
17266
References
- Rasche V, Oberhuber A, Trumpp S, Bornstedt A, Orend KH, et al. (2011) MRI assessment of thoracic stent grafts after emergency implantation in multi trauma patients: a feasibility study. EurRadiol21(7):1397-1405.
- Oberhuber A, Schabhasian D, Kohlschmitt R, Rottbauer W, Orend KH, et al. (2015) The bird beak configuration has no adverse effect in a magnetic resonance functional analysis of thoracic stent grafts after traumatic aortic transection. J Vasc Surg 61: 365-373.


