Keywords
Cranium-cerebral lesions, human brain, terminal ballistics, wound ballistics.
Introduction
Ballistics is the study of the firing, flight and terminal effects of projectiles. It is separated into three main stages: (a) internal ballistics or the study of projectile firing, (b) external ballistics or the description of projectile flight, and (c) terminal ballistics or the science of the projectile effect on the target.
The sector of internal ballistics studies the projectile’s motion within the weapon. There are three basic determinants of the exit velocity of the bullet: the mass of the bullet, the amount of the gunpowder in the cartridge and the length of the barrel.
The sector of external ballistics studies the projectile’s flight through the atmosphere as it travels towards its target. In this phase, the bullet is in a state of deceleration by virtue of the atmospheric drag effect. Moreover, the bullet undergoes several complex motions during its path [1].
The sector of terminal ballistics studies the damages in the target that result from missiles and modern arms of battle that enter into this [1,2]. There are many variables that describe the wounding potential of firearms, including weapon type and design, bullet type and target tissue characteristics. When the missile reaches the human organism, it is caused damage either by the entire missile either by its items. With the missile’s hitting, the permanent cavity is caused, while the temporary cavity is shaped by the continuous forward acceleration of air immediately afterwards the missile, forcing the cavity to be tensed externally. The shock waves compress the air and "travel" front the missile, as well as the sides and can reach up to 200 atm (≈ 2–107 Pa) pressure [3].
The present work examines the mechanisms of wound ballistics, the zones of missile’s way and the missile’s effect in the cranium. It should be referred that the direct medical and nursing intervention is essential that aims at the prevention of complications of cranium-cerebral lesions, which threaten the life of wounded person, as well as the complete cure of head’s lesions in interval of months or even years.
Ballistic Wound Mechanisms
There are four basic parameters that contribute the missile’s wound. However, none of these is always liable for the death or the weakening of the wounded person. These parameters are essential for the comprehension of damages, which a missile causes in the human organism [4]. They are filed in four categories:
(a) Penetration medium: is the tissue from which the missile passes and it is possible to displace or to destroy it (Figure 1).
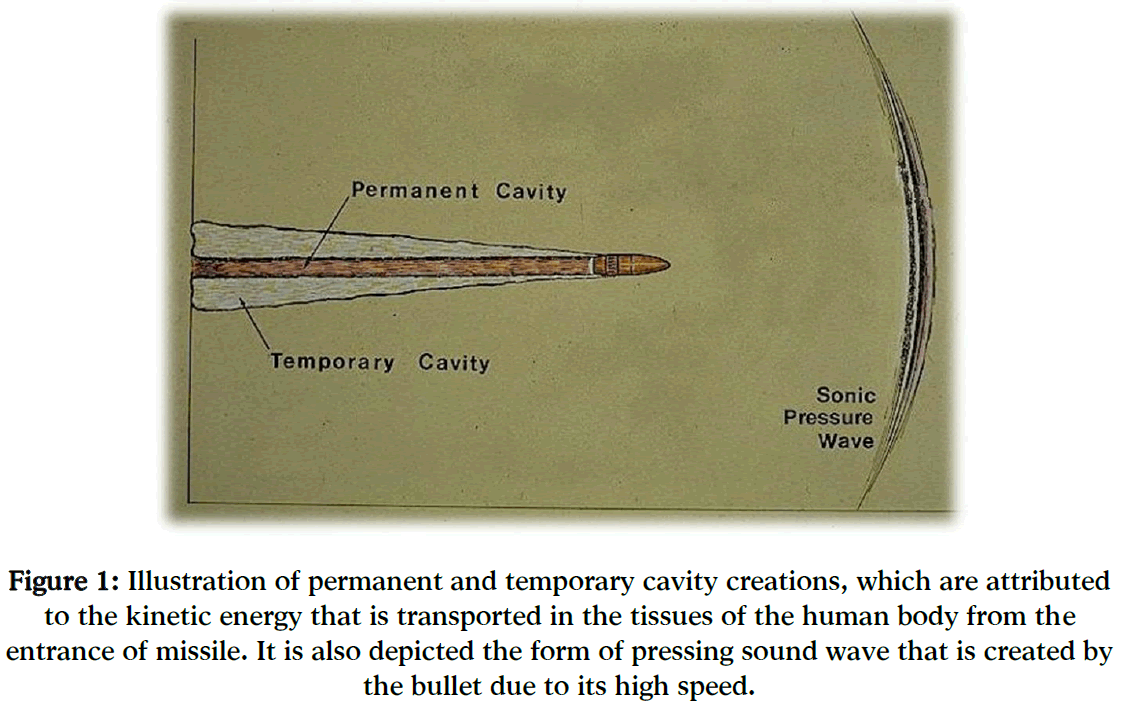
Figure 1: Illustration of permanent and temporary cavity creations, which are attributed to the kinetic energy that is transported in the tissues of the human body from the entrance of missile. It is also depicted the form of pressing sound wave that is created by the bullet due to its high speed.
(b) Permanent cavity: is the volume of space in the human body that was occupied by tissue, which was destroyed due to the way of missile’s entry (Figure 1). This volume depends on the penetration medium and the morphology of missile. Consequently, the permanent cavity is the aperture that the bullet creates, while it passes in the interior of the human body [4,5].
(c) Temporary cavity: is the extension of permanent cavity by virtue of the kinetic energy that is transported in the tissues by the missile.
(d) Fragmentation: is called the missile’s pieces or fragments from bones, which are prompted away from the permanent cavity and can offend neighbouring tissues, vital systems and blood vessels. The fragmentation is not observed in all missile’s wounds [4,6,7].
Zones of missile’s way
After the detonation, the missile’s way, proportional to its speed, is discriminated into three zones that vary on different arms: (a) rupture’s zone, (b) perforation’s zone and (c) fracture’s zone.
At the rupture’s zone, wounds are created due to the big missile’s speed and to the revolving movement, which places in movement the liquids of tissues and as a result the movement propagates circularly and multiples. Consequently, the entry’s wound (namely the wound, which is created due to the missile’s contact with the human tissues) is equal or smaller than the missile’s size (Figure 2), except for wounds that were created from absolute contact or minimum distance. The exit’s wound (namely the wound, which is created in the body’s interior at the exit of missile from the human body) is much bigger than the missile’s size (Figure 3). The duct of wound has a truncated cone figure with the base turned to the exit’s orifice. In order to be shaped the rupture’s zone, the missile should have speed bigger than 60 m/s.

Figure 2: Depiction of entry’s wound, which is equal or smaller than the missile’s size.
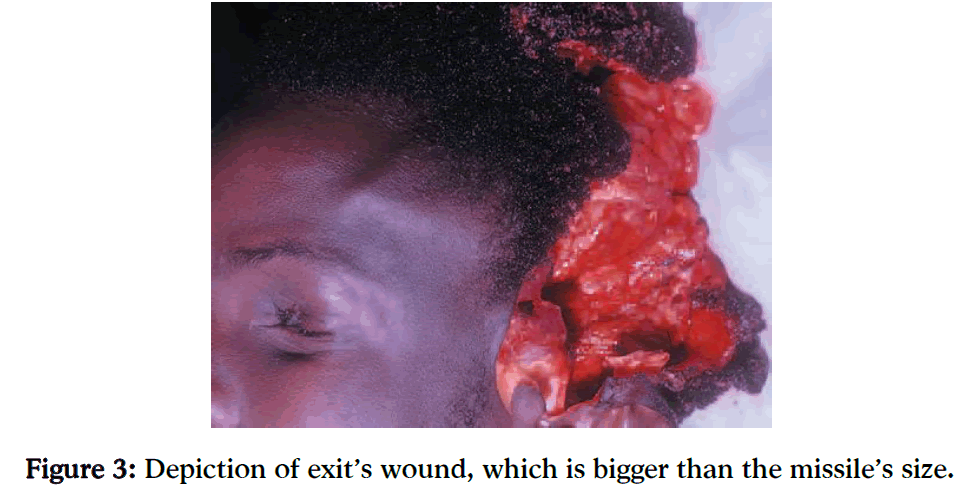
Figure 3: Depiction of exit’s wound, which is bigger than the missile’s size.
At the perforation’s zone, rupture’s wounds are not created, because the revolving movement of missile is absent. The entry’s orifice is equal or smaller than the missile’s diameter, while the exit’s orifice initially is double than the entry’s orifice, but at the end of perforation’s zone the exit’s orifice is equalized with the entry’s orifice. The duct of wound has a cylindrical figure.
The fracture’s zone begins from the end of perforation’s zone and reaches up to the missile’s fall. At this zone the missile maintains small speed and as a result does not cause wounds in the tissues, but simply fracture [8,9].
Missile effects at the cranium
The importance of wounds depends not only on the systems of the human organism that are affected, but also on the characteristics of missile that offend them. The missile’s spinning momentum has big relation with the way that the damage is caused, when the missile strikes the cranium. A missile of small caliber diameter, which is moved with high speed, begins to palpitate fast while it enters in the tissues, forcing more tissues to be moved. With this way, the bigger part of missile’s kinetic energy is transmitted in the cranium. A heavier missile of bigger caliber diameter transports more kinetic energy in the human body, even from bigger distance.
But, the missile can probability puncture so much the cranium and as a result to penetrate it with the rest of the kinetic energy. In addition, a missile with low kinetic energy can cause important damage at the cranium, if it is drawn to transport all its energy on the target.
Essential condition, however, is the near distance of the shot [10].
Moreover, the missile’s planning determines significantly the wound’s importance. The convention of Hagen and consecutively Geneva prohibit the use of explosive missiles in war time. This is the reason, why the military missiles are metal casing. In our days, the missiles have casing of copper, because the missiles begin to be made red-hot by the heat, which is produced in speeds bigger than 200 ft/s (approximately 61 m/s). A missile, which is sharp and small in diameter, can penetrate the human body and cause damage equal with a knife or a lance. The missile’s tip, drawn in order to destroy human tissues, should have a "brake", so as to transport all the kinetic energy at the target [11].
In addition, the missile’s speed plays an important role. The speed that ought to have a missile in order to penetrate the skin is 163 ft/s (almost 50 m/s) and in order to penetrate a bone is 213 ft/s (at about 65 m/s). Both values are low enough to cause damage at the cranium, but in combination with other factors, which were analyzed in the previous sections, can possible cause instantaneous death or various serious pathological situations, which are potentially dangerous in the future and require direct and correct confrontation. The most significant pathological situation is the cranium-cerebral lesion, which is analyzed extensively in the following section [12,13].
Cranium-Cerebral Lesions
The cranium-cerebral lesions are created when the head gets powerful knock or when in the battlefield a missile penetrates the cranium and enters into this. As a result, the wound can bring about locomotion of brain in the cranium, causing rupture of blood vessels and consequently profuse cerebral hemorrhage [14].
When a compressive fracture of cranium happens, it is possible to be developed hematoma, fracture or rupture of the cerebral tissue with all the inflammatory activities that are presented in each wound. One minor fracture of head can cause concussion. The concussion is term, which is used in order to describe a closed cranium-cerebral lesion at which there is disturbance of conscience’s level of short duration, amnesia relative with the event and headache [15].
In the cerebral fracture, the brain’s tissues are mauled, the blood is added up from the destroyed blood vessels and it is possible to be developed swelling, which causes increased pressure into the cranium [15,16].
The hematoma under the hard meninx is a usual result of cranium-cerebral lesion. The hematoma is swelling from blood. A missile that penetrates the head can cause rupture of blood vessels, which are found between the thin spidery membrane that covers the brain and the hard fibrous meninx. While the blood gushes under the hard meninx, the hematoma is increased in size, pressing the softer spider meninx and the cerebral tissue that the meninx covers.
The hematoma up the hard meninx happens rarely. When it happens, it is caused from rapid leak of blood from the medium of meninx’s artery and as a result the pressure into the cranium is increased. It recommends urgent medical situation. In order to be corrected the damage in the destroyed vessel and to be eased the rapidly developing pressure, before the death befalls by virtue of the increased pressure into the cranium, it must be executed incision at the cranium [17,18,19].
The exterior symptoms of cranium-cerebral lesion are enough obvious. These symptoms are the ecchymosis, the swelling and the haemorrhage. It is possible to be found fractures with ecchymosis or ecchymosis behind the ear. In addition, it can be observed effusion of liquid from the ear or the nose, difficulty in the sense of hearing, paralysis of face’s muscles and declination of eyes to a side. The effusion of liquid from the ear or the nose should be examined further in order to be determined if there is effusion of cerebro-spinal liquid.
In the points of the hematoma up the hard meninx are included the loss of senses, one short lucid interval that is followed by reduction of conscience’s level, headache, nausea and vomiting. The patient should be watched for points that mean increase of pressure into the cranium and for other points that mean damage in the brain [20].
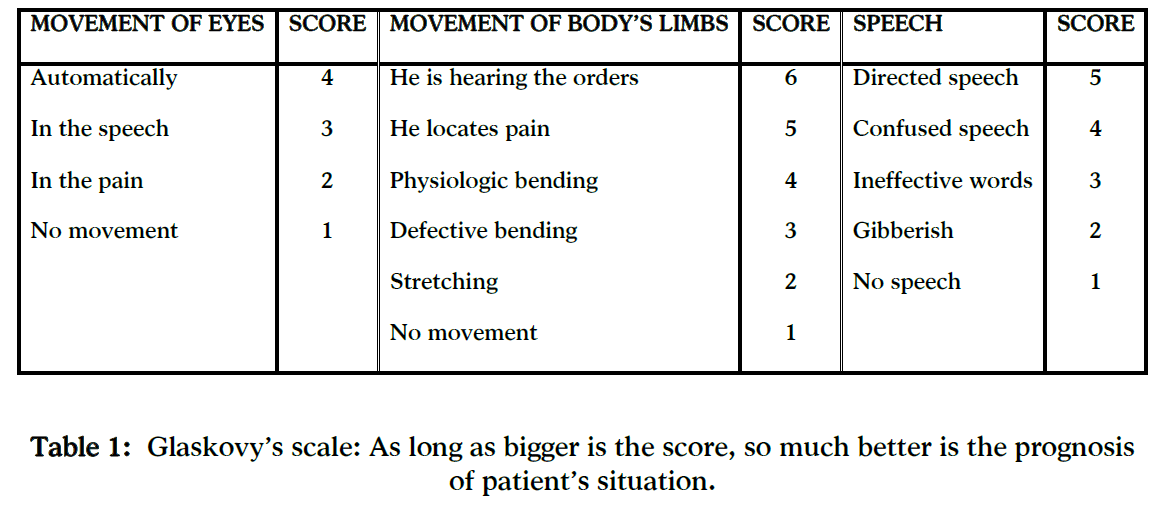
The Glaskovy’s scale (Table 1) is a diagnostic means of prognosis recognition based on the importance of cranium-cerebral lesions and brain’s wounds. As long as bigger is the score, so much better is the prognosis of patient’s situation.
The diagnostic tests that are usually used for the determination of extent of a cranium-cerebral lesion are the cranium’s radiograph, the axial tomography, the magnetic tomography, the tomography of positrons emission and the electroencephalogram [14,21,22].
The nursing intervention is considered very important for the control and treatment of cranium-cerebral lesions. If the nurse locates leak of cerebro-spinal liquid from the nose, the ear or the open wound, he ought to inform the doctor and take special measures for the prevention of wound’s contamination [23]. The precautionary measures include the following:
(a) The patient should remain absolutely laid up with the bed’s head raised at 30 until 45 deg, in order to be promoted the venous channelling from the head.
(b) The ear, by which the liquid effuses, should be covered with sterilized gauze, which should be changed periodically, so as the extent of channelling to be watched.
(c) The patient should be advised not to give his nose a blow and to avoid the contact with the hands. The blow can increase the pressure into the cranium and the contact with the hands can cause the entrance of micro-organisms.
(d) The nurse reminds to the patient that he should not change place in the bed for the prevention of increase of pressure into the cranium [24].
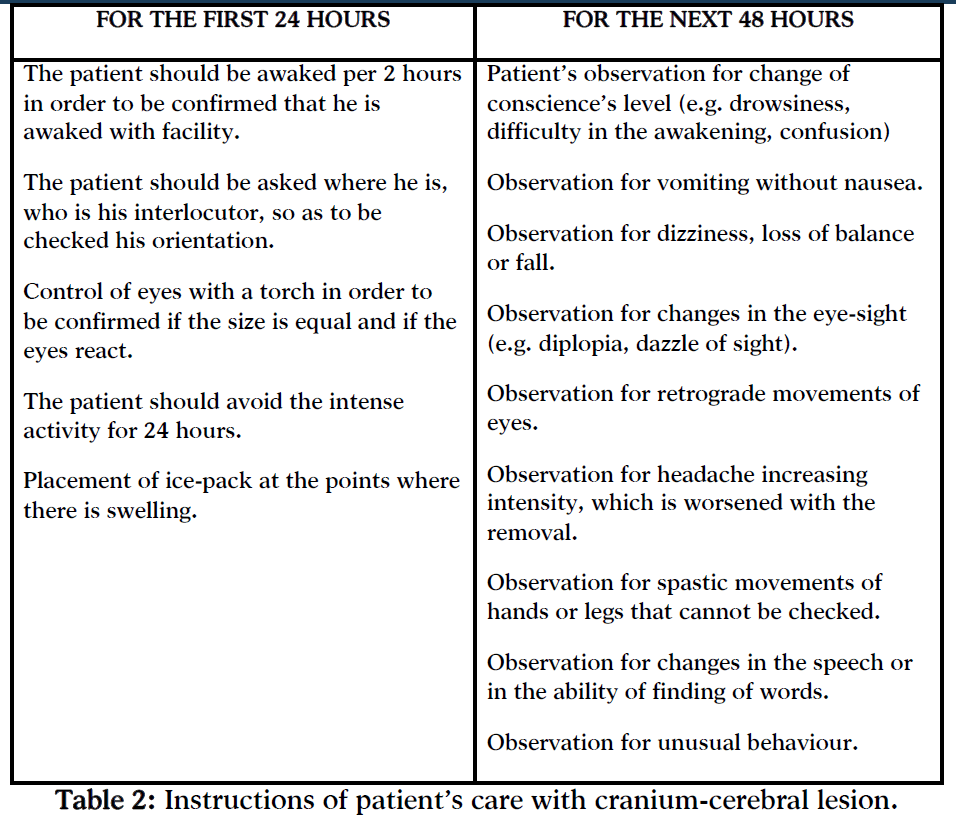
The observation of patient, who is in the department of urgent incidents by virtue of cranium-cerebral lesion and returns in the house, requires specifics instructions. These instructions are given to the family of the wounded person (Table 2) [25,26].
Conclusion
According to the above analysis, which was held in the previous sections, it is obvious that the factors that determine the importance of cranium wounds depend on the missile’s characteristics and on the characteristics of cranium’s tissues that are affected. As long as bigger are the speed and the missile’s mass, the form and the deceleration into the cranium, so much bigger is the opening up of the permanent cavity and bigger the wound. The kind of tissue, which is affected, is a decisive factor for the survival of the wounded person. The brain’s wound is usually incompatible with the life. Each scientist in the sector of health ought to know the way in which the missile enters the cranium so as to be able to face the wound immediately and effectively.
The cranium-cerebral lesions are brain’s damages, which are caused by knocks at the head or by the missile’s entrance into the cranium. They cause loss of conscience for hours or some days, which is followed by loss of memory. The cranium is possible to have fracture and it is possible to be developed hematoma into the cranium, up or under the hard meninx. As a result, these hematomas compress the brain and the pressure into the cranium is increased. The hematomas are recognized by the neurologists and the neurosurgeons with diagnostic tests that were referred in the previous sections.
The long-lasting outcome of patients with serious cranium-cerebral lesion is unexpected. The recovery is a long process and in some patients the improvement can happen after a lot of months. It is also possible the infirmities to remain forever. In every case, the direct medical and nursing intervention is essential that aims at the prevention of complications of cranium-cerebral lesions, which threaten the life of wounded person, as well as at the complete cure of head’s lesions in interval of months or even years.
3324
References
- Thali M.J., Kneubuehl B.P., Zollinger U., Dirnhofer R. A Study of the Morphology of Gunshot Entrance Wounds in Connection with their Dynamic Creation, Utilizing the "Skin–Skull–Brain Model". Forensic Sci Int. 2002; 125:190–194.
- Alexandropoulou C.E., Panagiotopoulos E.E. Traumatic Ballistics: Analysis of Parameters and Confrontation of Wounds Caused from Missiles in Human Body. Hellenic Journal of Nursing Science. 2009; 2(2):30-34.
- Korac Z., Kelenc D., Hancevic J., Baskot A., Mikulic D. The Application of Computed Tomography in the Analysis of Permanent Cavity: a New Method in Terminal Ballistics. Acta Clin Croat. 2002; 41:205–209.
- Alexandropoulou C.E., Panagiotopoulos E.E. Traumatic Ballistics: Analysis of Pathological Situations and Confrontation of Wounds Caused from the Entrance of Missiles in the thoracic cavity. Hellenic Journal of Nursing Science. 2009; 2(3):53-57.
- Alexandropoulou C.E., Panagiotopoulos E.E. Wound Ballistics: Analysis of Blunt and Penetrating Trauma Mechanisms. Health Science Journal. 2010; 4(4):225-236.
- White K.M. Injuring Mechanisms of Gunshot Wounds. Crit Care Clin North Am. 1989; 1:97-103.
- Faller-Marquardt M., Bohnert M., Pollak S. Detachment of the Periosteum and Soot Staining of its Underside in Contact Shots to the Cerebral Cranium. Int J Legal Med. 2004; 118:343–347.
- Karger B., Banaschak S. Two Cases of Exenteration of the Brain from Brenneke Shotgun Slugs. Int. J. Legal Med. 1997; 10:323–325.
- Suwanjutha T. Direction, Site and the Muzzle Target Distance of Bullet in the Head and Neck at Close Range as an Indication of Suicide or Homicide. Forensic Sci. Int. 1988; 37:223-229.
- Courtney A., Courtney M. Links between traumatic brain injury and ballistic pressure waves originating in the thoracic cavity and extremities, Brain Inj., 2007; 21(7): 657-662.
- Oehmichen M, Meissner C, Konig H.G, Gehl H.B. Gunshot Injuries to the Head and Brain Caused by Low-Velocity Handguns and Rifles: A Review. Forensic Sci Int. 2004; 146:111–120.
- Goransson A.M., Ingvar D.H., Kutyna F. Remote Cerebral Effects on EEG in High-Energy Missile Trauma. The Journal of Trauma. 1988; 204-205.
- Thali M.J., Kneubuehl B.P., Vock P., Allmen G., Dirnhofer R. High-Speed Documented Experimental Gunshot to a Skull-Brain Model and Radiologic Virtual Autopsy. Am J Forensic Med Pathol. 2002; 23:223–228.
- Susan C. deWit. Medical-Surgical Nursing: Concepts and Practice. The patient with cranium-cerebral lesions and lesions of spinal column. Texas: Saunders Elsevier Inc; 2009:749-757.
- Prahlow J.A., Barnard J. Contact Gunshot Wound of the Head: Diagnosis with Surgical Debridement of the Wound. J. Clin. Forensic Med. 1999; 6:156–158.
- Faller-Marquardt M., Pollak S. Skin tears Away from the Entrance Wound in Gunshots to the Head. Int J Legal Med. 2002; 116:262–266.
- Johnson G.C. Unusual Shotgun Injury – Gas Blowout of Anterior Head Region. Am. J. Forensic Med. Pathol. 1985; 6(3):244–247.
- Jacob B., Barz J., Haarhof K., Sprick C., Worz D., Bonte W. Multiple Suicidal Gunshot Wounds to the Head. Am J Forensic Med Pathol. 1989; 10:289.
- Prahlow J.A., McClain J.L. Lesions that simulate gunshot wounds. J. Clin. Forensic Med., 1997; 4: 121–126.
- Alexandropoulou C.E., Panagiotopoulos E.E. Clinical Symptoms of cranium-cerebral lesions caused by the entrance of missiles in the cranium of the human body and nursing confrontation. Hellenic Journal of Nursing Science. 2009; 2(4):74-77.
- Steyerberg E.W., Mushkudiani N., Perel P. Predicting outcome after traumatic brain injury: development and international validation of prognostic scores based on admission characteristics, 2008.
- Perel P., Arango M., Clayton T. Predicting outcome after traumatic brain injury: practical prognostic models based on large cohort of international patients, 2008.
- Alexandropoulou C.E., Panagiotopoulos E.E. Wound Ballistics: Analysis of Pathological Situations Caused at the Thoracic Cavity and the Cranium of the Human Body by the Missile's Entrance, 4-7 Nov 2010, Makedonia Palace, Thessaloniki: Army General Staff.
- Snow A.F., Bozeman J.M. Role implications for nurses caring for gunshot wound victims, Crit Care Nurs Q., 2010; 33(3): 259-264.
- Shuker S.T., Sadda R. Craniomaxillofacial falling bullet injuries and management, J Oral Maxillofac Surg., 2010; 68(7): 1593-1601.
- Koehler S.A. Firearm evidence and the roles of the ER nurse and forensic nurse, J Forensic Nurs., 2009; 5(1):46-48.

